How Much Does a Podiatry Clinic Owner Make? $240K Salary Plus Profit
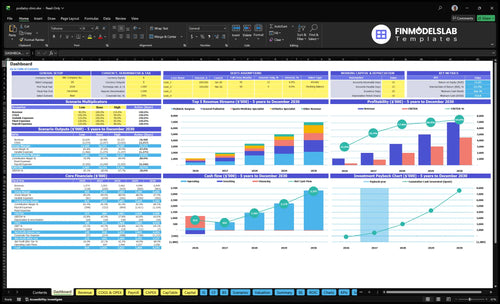
You’re modeling owner income, not just a podiatrist job salary This five-year plan shows $1074 million in Year 1 revenue, $277,000 in Year 1 EBITDA, and a $240,000 medical director salary before personal taxes, debt service, reserves, or reinvestment By Year 5, revenue reaches $6949 million with $4490 million in EBITDA under the stated provider, volume, and capacity assumptions
Owner income$240k+Net margin25.8% to 64.6%Revenue for target pay$930kBusiness difficultyHard
Want to test your podiatry clinic income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
How does the Podiatry Clinic model show owner income?
Is owning a podiatry clinic more profitable than being employed?
Owning a Podiatry Clinic can be more profitable than employment because the model includes a $240,000 medical director salary plus clinic EBITDA of $277,000 in Year 1 and $4,490 million in Year 5, but that upside carries real execution risk. Employment gives salary certainty; ownership only wins if collections, provider capacity, and reinvestment stay on plan, so track the right numbers early with What 5 KPIs Should Podiatry Clinic Track?.
Owner upside
$240,000 medical director salary
$277,000 Year 1 clinic EBITDA
$4,490 million Year 5 clinic EBITDA
Profit rises with provider utilization
Owner risk
$733,000 minimum cash need
$343,000 startup capex
Staff hiring and rent pressure
Collections lag can erase upside
What is a good profit margin for a podiatry clinic?
If you’re sizing a Podiatry Clinic, a good margin is the one that still holds after direct clinic costs and overhead; the source model shows EBITDA margins of 258% in Year 1, 454% in Year 2, 578% in Year 3, 608% in Year 4, and 646% in Year 5, with setup context here: How Much To Start A Podiatry Clinic?. Gross margin is the layer before overhead, operating profit comes after the $23,500 monthly fixed base, and cash flow can still trail EBITDA because of capex, debt, and reserves. Owner distributions are what’s left after that, so the real squeeze is on medical supplies, orthotics and DME inventory, billing fees, and card fees.
Margin layers
EBITDA: 258% to 646%.
Gross margin comes before overhead.
Operating profit follows fixed costs.
$23,500 monthly fixed expenses matter.
Cash reality
Medical supplies: 60% to 70%.
Orthotics and DME: 50% to 60%.
Billing fees: 40% to 50%; card fees: 25%.
Cash flow can lag EBITDA; distributions come last.
Can a solo podiatry clinic owner make more by adding providers?
Yes—a solo owner can make more in a Podiatry Clinic, but only if added providers stay busy enough to cover payroll and support costs. In this model, provider roles grow from 4 in Year 1 to 11 in Year 5, with revenue rising from $1.074 million to $6.949 million and EBITDA from $277,000 to $4.49 million.
Where income scales
More visits lift owner profit.
More roles expand service mix.
General podiatrists add volume.
Surgeons and wound care deepen revenue.
What can hurt margins
Hiring early can outpace demand.
More MAs and front desk staff raise costs.
Billing gets heavier fast.
Low utilization kills the upside.
Want the six main income drivers?
1
Patient Volume
2.4K/mo
Year 1 starts at 2,395 effective monthly treatments and $1.074M revenue, then grows to $6.949M by Year 5.
2
Payer Mix
26%-65%
Better payer mix and fewer write-offs widen EBITDA, or cash profit before taxes and reinvestment, from about 26% in Year 1 to 65% in Year 5.
3
Service Mix
$165-$1.5K
A heavier mix of surgery and orthotics lifts ticket size because prices range from $165 to $1,500 per treatment.
4
Provider Output
60-240/mo
More visits per clinician spread wages across more treatments, so the same team can generate more take-home cash.
5
Overhead Control
$23.5K/mo
Fixed overhead stays at $23,500 a month, so every extra dollar of gross profit flows to owner income before taxes and reinvestment.
6
Billing Quality
6.5%-7.5%
Billing and card fees run about 6.5% to 7.5% of revenue, so cleaner claims and faster follow-up keep more cash in the clinic.
Podiatry Clinic Core Six Income Drivers
Patient volume and clinic capacity
Patient volume and clinic capacity
When schedules fill, income rises faster than rent and payroll. Year 1 effective monthly volume is 27 surgeon treatments, 110 general podiatry visits, 64 sports medicine visits, and 385 orthotics treatments; by Year 5 it reaches 119, 864, 306, 1,445 wound care, and 208 orthotics treatments. No-shows cut collections without cutting fixed cost, so the real gain comes from filling more slots.
Here’s the quick math: moving utilization from 35% to 50% lifts revenue by using the same rooms, staff, and hours more often. Mature operations need 80% to 90% utilization to support stronger owner pay, but only if referral flow and scheduling stay steady. If capacity grows but booked visits do not, EBITDA stays tight.
Track filled slots, not just booked visits
Measure available slots, kept visits, no-show rate, and referral volume by provider and service line. Keep a daily view of utilization so you can see which visit types are underfilled before they drag cash flow. One clean rule: empty chairs are lost revenue, but the rent still clears.
Track kept visits by provider.
Watch no-shows by service line.
Compare referrals to open capacity.
Forecast pay from filled schedules.
If one specialty fills faster than the rest, shift slots there first. That protects margin because fixed payroll and rent do not move much month to month, while each extra kept visit adds direct revenue and improves the owner’s distribution capacity.
1
Net collections and payer mix
Net collections and payer mix
Use collections, not billed charges, because that is the cash that pays payroll, rent, and owner draw. In this model, net collection prices start at $165 for general podiatry in Year 1 and rise to $1,350 for surgery and $450 for orthotics; by Year 5 they move to $185, $1,500, and $510.
Here’s the quick math: if payer mix, contracted rates, patient responsibility, denials, and collection discipline slip, the same visit volume can still miss plan. Every unpaid claim cuts EBITDA and owner distributions, so high volume does not guarantee cash. This driver is mostly about cash conversion speed and the percent of allowed charges that actually lands in the bank.
Track cash, not charges
Measure net collection rate, denial rate, patient balance collection rate, and days in accounts receivable. Use them by service line, since surgery, general care, and orthotics all collect at different levels. Track the gap between expected allowed amount and actual cash, because that gap tells you where profit is leaking.
Test payer mix before adding volume. If contracts are weak or patient collections lag, higher scheduling only grows work, not take-home pay. One clean rule: if collections fall, owner pay falls. Tight billing follow-up and front-end payment checks protect EBITDA more than chasing more billed charges ever will.
2
Service and procedure mix
Service and procedure mix
This driver is the mix of surgery, general care, sports medicine, orthotics, and wound care, and it changes average net collection per visit. In Year 1, surgery is $1,350, general care $165, sports medicine $275, and orthotics $450; wound care starts in Year 2 at $235. A more procedure-heavy mix can lift revenue per appointment, but it also changes cost structure fast.
Here’s the quick math: if 60% of medical supply cost and 50% of orthotics and DME inventory flow through COGS, higher-ticket services do not equal higher profit unless gross margin holds. The owner’s take-home rises when collected revenue grows faster than supplies, inventory, and staffing. What this estimate hides: payer mix and no-shows can still flatten cash.
Measure margin by service
Track visits by service line, collected dollars per visit, and supply cost per case. The key inputs are appointment mix, net collection rate, and inventory use. If surgery and orthotics expand without tight purchasing, gross margin can shrink even as sales rise. One clean rule: watch contribution by service, not just volume.
For planning, compare each procedure’s net collection against direct cost before adding fixed overhead like rent and payroll. In a small clinic, a shift from general care to higher-value procedures can improve owner draw only if cash comes in fast and stock turns cleanly. If supply usage creeps up, the extra revenue may never reach profit.
3
Provider productivity and staffing leverage
Provider productivity
Provider productivity is the revenue each podiatrist or specialist can collect from a full, well-run schedule. Here’s the quick math: revenue per provider role is about $269,000 in Year 1 and $632,000 in Year 5, so owner income rises only when each clinician sees enough billable visits to cover support labor and clinic overhead.
What this hides: hiring too early can shrink take-home pay. The staffing stack includes $240,000 for a medical director, $85,000 for a clinic manager, $48,000 for medical assistants, $42,000 for front desk coordinators, and $55,000 for billing specialists, so added associates help only when schedules fill and throughput stays clean.
Fill schedules before adding staff
Track booked visits per provider, kept visits, no-show rate, and collections per clinician each month. If schedules are thin, add demand first; if rooms turn fast and support keeps pace, a new associate can spread fixed labor across more visits and lift owner distributions.
Booked visits per provider
No-show and cancellation rate
Collections per clinician
Support labor per provider
Open time between visits
The test is simple: does one more provider add more collected revenue than the full labor cost needed to support that schedule? If not, payroll rises faster than cash, and profit gets trapped in staffing instead of flowing to the owner.
4
Overhead and fixed-cost control
Overhead Control
Overhead is the fixed bill that shows up whether the schedule is full or not. Here it totals $23,500 per month: $12,000 rent, $3,500 malpractice insurance, $1,200 software, $4,000 marketing, $1,500 utilities, $800 maintenance, and $500 office supplies. That base raises break-even and cuts owner pay because profit has to clear this stack before any draw.
The key test is overhead per completed visit. If monthly collections or utilization slip, the fixed base does not move, so cash gets squeezed fast. The $343,000 clinic buildout and equipment base also matters: every room, machine, or system should support booked patient flow. If it does not, it becomes expensive idle capacity.
Cut the Fixed Base
Track fixed costs as a share of collections and review each line every month. If a cost does not help fill schedules, support care, or improve cash collection, trim it. The goal is to keep the $23,500 base low enough that owner pay can start sooner, even while patient volume is still ramping.
Stage equipment buys, avoid empty rooms, and tie marketing spend to booked visits, not just leads. What this estimate hides is simple: unused overhead burns runway. Lower unused overhead protects cash during early ramp-up and leaves more profit available for the owner once the clinic starts filling its schedule.
5
Billing and collections performance
Billing and collections performance
In a podiatry clinic, billing and collections turn visits into usable cash for payroll, reserves, and owner pay. If billing and collection fees run at 50% of revenue in Years 1 and 2, then 45% in Year 3 and 40% later, cash conversion matters as much as volume. Delayed collections can trap EBITDA in A/R instead of paying the owner.
Track clean claim rate, denial rate, accounts receivable aging, patient balances, and collection rate. Card and transaction fees stay at 25%, so weak collections hit margin fast. Here’s the quick math: if cash lags, the clinic may look profitable on paper but still run short on distributable cash.
Measure cash, not just charges
Use net collections as the main lens. Compare billed charges to cash collected each month, then break out payer, patient, and card fees so you can see where margin leaks. If A/R aging rises or patient balances stack up, owner distributions usually fall even when visits stay strong.
Set a monthly review for clean claims, denials, and collection rate. Push for faster payment on patient balances and watch fee load against revenue, since 50% billing and collection costs in early years leave little room for delay. The goal is simple: collect faster so profit turns into cash the owner can actually use.
Clean claim rate: first-pass payment speed
Denial rate: cash lost to rework
A/R aging: slow cash warning
Patient balances: owner-pay risk
Collection rate: real cash yield
6
Compare podiatry clinic owner income scenarios
Owner income scenarios
Owner income rises as provider count, visit volume, and pricing scale. Early pay is salary-led; later years add EBITDA, but payroll, overhead, reserves, and distribution policy decide what reaches the owner.
Compare lean, scaled, and mature owner pay cases.
Scenario
Low CaseRamp-up
Base CaseScaled
High CaseMature
Launch model
This is a lean ramp-up path where owner pay is mostly salary.
This is the scaled case where salary and profits both matter.
This is the mature case where stronger EBITDA supports bigger owner pay.
Typical setup
Year 1 uses 4 provider roles, $1.074M revenue, and $277k EBITDA, which is a 25.8% margin, with Month 2 break-even and the owner in a $240k salary role.
Year 3 reaches 7 provider roles, $3.462M revenue, and $2.001M EBITDA, which is a 57.8% margin, so owner income can support salary plus a larger profit draw if payroll stays tight.
Year 5 reaches 11 provider roles, $6.949M revenue, and $4.490M EBITDA, which is a 64.6% margin, but reserve needs and distribution policy still matter as staffing scales.
Cost drivers
4 provider roles
$1.074M revenue
25.8% EBITDA margin
$240k owner salary
Month 2 break-even
7 provider roles
$3.462M revenue
57.8% EBITDA margin
payroll scale
overhead control
11 provider roles
$6.949M revenue
64.6% EBITDA margin
reserve needs
distribution discipline
Owner income rangeBefore owner reserves
$240,000 salarySalary-led
Salary + profit drawProfit draw
Salary + larger drawUpside draw
Best fit
Use this to stress-test the opening-year cash and pay mix.
Use this as the planning case for a growing clinic.
Use this to test upside once the clinic is fully scaled.
!
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution outcomes.