How Much Can A Psoriasis Treatment Center Owner Make? $280K To $37M
This five-year model separates clinic profit from owner salary, distributions, and reinvestment reserves In the researched base case, the center moves from $94,320 in monthly revenue and -$133,126 EBITDA in Year 1 to $523,372 in monthly revenue and $3423 million EBITDA in Year 5 Owner take-home depends on whether the owner is the dermatologist, how much profit is reserved, and whether debt service applies
Owner income$280k baseNet margin-118% to 545%Revenue for target pay$3.1MBusiness difficultyHard
Want to test your owner pay target?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: This output is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
Want to see the income model for Psoriasis Treatment Center?
Does a psoriasis treatment center owner need to be a dermatologist?
No. A Psoriasis Treatment Center can be owned by a non-dermatologist, as long as clinician hiring, supervision, and state licensing are handled correctly in the US. If the owner is the dermatologist, the $280,000 salary line can be owner pay; if the dermatologist is hired, that salary becomes payroll and the owner takes profit distributions instead.
Ownership
Owner dermatologist: salary can be pay.
Hired dermatologist: salary is payroll.
Owner income then comes from distributions.
Keep US supervision rules general.
Staffing
Year 1: 1 dermatologist, 1 physician assistant.
Year 5: 3 dermatologists, 2 physician assistants.
Plan hiring around treatment demand.
Match payroll to visit volume.
How many patients does a psoriasis treatment center need to pay the owner?
A Psoriasis Treatment Center with 369 completed monthly treatments and $94,320 in monthly revenue is not yet paying the owner; it still has to cover $22,800 a month in overhead, $889,500 a year in payroll, and about 90% in combined COGS and variable costs. Here’s the quick math: payroll alone is about $74,125 per month, so collections need to be much higher before any owner draw starts.
Break-even math
$94,320 monthly revenue at 45% capacity
$1,131,840 annual revenue at current pace
$22,800 monthly overhead, or $273,600 yearly
$889,500 yearly payroll before owner pay
Cash risks
No-shows reduce completed treatments
Prior authorization delays slow collections
Owner distributions come after break-even
Target completed treatments, not booked visits
How much can a psoriasis treatment center owner make?
A Psoriasis Treatment Center owner can make $280,000 in modeled dermatologist pay if they work clinically, but owner distributions only make sense after positive cash flow; How To Write A Business Plan For Psoriasis Treatment Center? should separate salary from profit payouts. Year 1 EBITDA is -$133,126, so extra distributions are not supported.
Owner Pay
Clinical owner pay: $280,000
Year 1 EBITDA: -$133,126
No Year 1 distributions supported
Cash flow controls payouts
Profit Upside
Year 3 EBITDA: $1.115 million
Year 5 EBITDA: $3.423 million
Figures are before taxes and debt
Nonclinical owners rely on distributions only
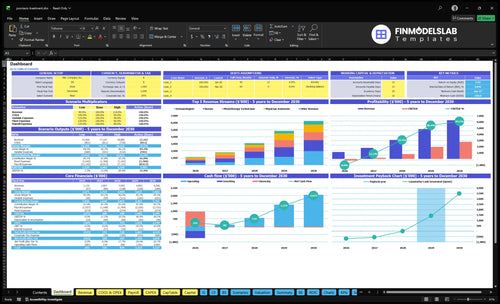
Psoriasis Treatment Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want to see the main income drivers?
1
Patient Volume
$94K-$523K/mo
More visits push monthly revenue from $94K to $523K and spread fixed costs thinner.
2
Provider Utilization
45%-85%
Capacity moves from 45% to 85%, so idle clinician time turns into billable output.
3
Service Mix
$110-$595
Visit mix changes price per treatment from $110 to $595, which moves margin fast.
4
Collections
M14
Faster collections keep cash moving and help the clinic reach breakeven in Month 14.
5
Staffing Costs
$890K-$2.09M
Payroll runs about $890K to $2.09M, so staffing adds or protects EBITDA fast.
6
Facility Overhead
$22.8K/mo
Fixed overhead holds at about $22.8K a month, and lean ops leave more for owner take-home.
Psoriasis Treatment Center Core Six Income Drivers
Patient Volume
Completed Visits
Revenue starts with completed visits, not booked names. In this model, 369 completed monthly treatments in Year 1 scale to 1,962 by Year 5, a 5.3x lift. Recurring follow-ups, flare visits, and treatment sessions raise revenue density because the same patient can generate multiple billable touches.
The risk is simple: booked demand that never gets collected. If no-shows, prior-auth delays, or unpaid balances block completion, the clinic can look busy but still miss cash. More completed care usually improves owner pay only after payroll and fixed overhead are covered, so empty slots hurt twice.
Fill the Schedule
Track scheduled-to-completed conversion, no-show rate, and treatment mix by provider type. Use capacity as the base: Year 5 only works at 85% capacity, so every room, chair, and staff hour needs a fill target. If a visit is not completed and collected, it should not count in the forecast.
Push reminders, same-week rebooking, and follow-up bundles so one patient fills more than one slot. Here’s the quick math: 1,962 monthly treatments at scale matter more than raw inquiries. What this hides is revenue leakage from authorizations and unpaid self-pay, so owners should reconcile booked, completed, and collected volumes each month.
1
Payer Mix And Collections
Collections Set Owner Pay
Owner income follows collected revenue, not billed charges. In Year 1, the model prices range from $550 per dermatologist treatment to $110 per medical assistant service, so denials, prior authorization delays, Medicare mix, commercial mix, and unpaid self-pay balances can cut cash fast. If collections slip, the same rooms and staff produce less take-home income.
Here’s the quick math: every visit still carries payroll and fixed overhead, but only the collected share funds profit. So a stronger collection rate lifts margin without adding rooms, because each paid treatment adds cash and each write-off just lowers owner draw. That matters most when treatment volume is growing but cash is not.
Track Net Collections, Not Billed Charges
Measure net collection rate, denial rate, prior auth lag, and self-pay aging by service line. Split results by dermatologist, physician assistant, nurse, phototherapy technician, and medical assistant visits so you can see where cash leaks. If billed volume rises but collected dollars do not, the problem is payer mix or billing discipline, not demand.
Use faster claim follow-up, clean prior auth, and point-of-service payment rules on self-pay balances. The goal is simple: raise collected revenue per treatment so owner pay grows faster than headcount, rent, and equipment use. Better billing often beats adding more rooms.
Track denial reasons weekly.
Age self-pay by 30 days.
Monitor Medicare and commercial mix.
Fix prior auth before treatment.
2
Service Mix
Service Mix
Service mix changes how much cash each staffed hour brings in. In Year 1, phototherapy contributes $14,400 a month, dermatologist services $24,750, and physician assistant services $20,520. By Year 5, phototherapy reaches $95,288, so the mix can shift revenue fast if rooms, staff, and equipment stay busy.
The catch is margin. Phototherapy only helps owner pay when volume covers technician payroll and equipment use. Biologic management should be modeled mainly as clinical visit revenue unless drug margin is counted separately, or profit will look too high.
Track revenue per service hour
Build the model from completed visits, price per service, provider hours, and equipment time. Add collections, not just charges, because owner income follows cash collected. One clean metric matters most: revenue per hour by service line.
Count completed sessions by type.
Track staff time per session.
Separate drug margin from visit revenue.
Watch technician payroll against phototherapy use.
If a service fills rooms but does not cover labor and equipment, cut or reprice it. That is where take-home pay gets protected.
3
Provider Utilization
Provider Utilization
Utilization is the share of provider and room capacity that turns into billable care. Here, it rises from 45% in Year 1 to 85% in Year 5, and that is the main lift behind monthly revenue growing from $94,320 to $523,372. That is a gain of $429,052 a month, before you even think about owner pay.
What drives it: schedule design, room turnover, no-shows, treatment batching, and staff count. If utilization lags, payroll and the $22,800 monthly fixed overhead get spread across fewer visits, so margin and cash get tight. Push it too hard, though, and care quality and follow-up access can slip.
Measure the Full-Day Fill Rate
Track booked time, kept visits, and completed treatments by provider type, not just inquiry volume. Compare actual utilization to the 45% to 85% path, and watch where gaps come from: late starts, open rooms, short fills, and cancellations. Here’s the quick math: each unused hour lowers revenue per payroll dollar and makes owner draw harder to support.
Improve this by batching treatments, tightening room handoffs, and confirming follow-ups before patients leave. Use waitlists to backfill cancellations, but don’t overbook to the point that access drops. The clean test is simple: if higher utilization raises revenue without hurting follow-up slots, collections, or care quality, it’s helping owner income.
4
Staffing Cost Structure
Staffing Cost Structure
Payroll is the biggest controllable cost in a psoriasis clinic, and it hits owner pay fast. Annual payroll is $889,500 in Year 1, then about $1.444 million in Year 3 and $2.094 million in Year 5. Key salaries include $280,000 per dermatologist, $115,000 per physician assistant, $90,000 per nurse, and $65,000 per phototherapy technician. Owner labor should sit outside hired payroll, or profit gets overstated.
Here’s the quick math: at Year 1 revenue of $94,320 a month, that payroll is about 79% of annualized sales. By Year 5, revenue rises to $523,372 a month, so payroll falls to about 33% of annualized sales. Overhiring before capacity fills creates margin drag and delays the cash you can take home.
Control Payroll Before Capacity Fills
Track payroll by role and tie every hire to filled schedules, not booked interest. Add expensive providers only when collected revenue can cover the added salary plus support labor. A $280,000 dermatologist or $115,000 physician assistant changes the cost base quickly, so use utilization and collections as the gate. If demand is uneven, part-time or mixed-role staffing protects margin better than adding full-time headcount too early.
Track collected revenue per staffed hour.
Separate owner hours from payroll.
Hire only when utilization stays high.
Watch idle phototherapy and nurse time.
5
Facility And Equipment Overhead
Fixed Facility Overhead
$22,800 in monthly fixed overhead sets the floor before any patient is seen: $12,000 lease, $4,500 malpractice insurance, $1,800 utilities, $1,200 equipment maintenance, and $1,200 medical record software. That cost hits income fast in the early ramp-up, because it must be covered before owner pay starts.
The $275,000 equipment buildout for phototherapy units, exam equipment, biologic storage refrigerators, and system setup is mainly a cash-flow issue. It ties up capital upfront, so even a healthy service mix can still leave the owner short on take-home cash if collections lag or volume starts slow.
Keep Fixed Costs Below Collected Margin
Track fixed overhead monthly and compare it with collected revenue, not billed charges. Here’s the quick math: until collections cover $22,800, the clinic is still funding the building, the insurance, and the software from cash reserves or owner capital. That means every delay in ramp-up pushes out the first real owner draw.
Watch these inputs closely:
Lease and renewal terms
Malpractice premium changes
Utilities and maintenance bills
Software fees and equipment downtime
Capex timing for new equipment
6
Psoriasis Treatment Center Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Scenario objective for lean, base, and high-performance owner income planning
Owner income scenarios
Owner income moves from no supported distributions in Year 1 to $1.115M in Year 3 and $3.423M in Year 5 as capacity, staffing, and pricing improve.
Low, base, and high owner income under the model.
Scenario
Lean CaseLean case
Base CaseBase case
High CaseHigh case
Launch model
This is the lower-income path, with Year 1 scale and thin early cash flow.
This is the modeled middle path, where Year 3 operations are scaled and owner income turns positive.
This is the stronger earnings path, with Year 5 scale and the highest modeled owner income.
Typical setup
Year 1 revenue is $1.132M, EBITDA is negative, capacity sits at 45%, and the clinic runs with one dermatologist and a small support team.
Year 3 revenue is $3.092M, EBITDA is $1.115M, capacity reaches 70%, and the clinic runs with two dermatologists plus broader support.
Year 5 revenue is $6.280M, EBITDA is $3.423M, capacity reaches 85%, and the clinic runs with three dermatologists and a larger support team.
Cost drivers
45% capacity
1 dermatologist
1 physician assistant
high payroll
3.0 marketing spend
70% capacity
2 dermatologists
1 physician assistant
3 nurses
2 technicians
85% capacity
3 dermatologists
2 physician assistants
4 nurses
4 medical assistants
Owner income rangeBefore owner reserves
No supported distributionsNo distributions
$1.115MBase income
$3.423MHigh income
Best fit
Use this to stress-test early demand and a salary-only owner take-home.
Use this as the main planning case for steady operations and normal growth.
Use this to test upside if the clinic fills capacity and keeps labor productive.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
If the owner is the dermatologist, the model includes $280,000 in clinical pay Extra distributions are not supported in Year 1 because EBITDA is about -$133,126 By Year 5, EBITDA reaches $3423 million before taxes, debt service, reserves, and reinvestment, so take-home depends on distribution policy
In this model, operating profit turns positive after the first year Year 1 EBITDA is -$133,126 on $1132 million revenue, while Year 2 EBITDA is about $394,571 on $1807 million revenue The swing comes from capacity rising from 45% to 60% while fixed overhead stays at $22,800 per month
Yes, plan reserves because insurance collections rarely match billed charges right away The model has $889,500 in Year 1 payroll, $273,600 in annual fixed overhead, and $275,000 in startup capex If claims lag or authorizations slow care, owner distributions should wait until payroll and vendors are safe
Capacity, collections, and payroll drive profit most Revenue rises from $94,320 per month in Year 1 to $523,372 in Year 5 as utilization moves from 45% to 85% Payroll also rises from $889,500 to $2094 million, so hiring must track completed visits, not just demand
Keep owner pay tied to cash flow, not optimism If the owner is the dermatologist, the $280,000 salary line may be reasonable, but Year 1 EBITDA is negative before reserves A safer plan is to defer distributions until monthly revenue covers payroll, $22,800 fixed overhead, COGS, and variable costs
About the author
Felix Ward
Entrepreneurship Researcher
Felix Ward is an entrepreneurship researcher at Financial Models Lab who focuses on expense and revenue planning for people opening a new small business. He turns practical business questions into clear planning steps, with a special focus on first-year business planning. Known for making business planning easier for non-finance readers, he writes in a calm, structured, and approachable way.
Choosing a selection results in a full page refresh.