How To Open A Psoriasis Treatment Center In 6–12 Months
Key Takeaways
Compliance must clear first, or launch slips and costs rise.
Dermatologist hiring drives opening date and early appointment capacity.
Payer credentialing protects cash flow, but slows first collections.
Ready workflows and equipment reduce cancellations and unpaid claims.
Time to Open12 monthsOpening prepLaunch Sequence8 stagesCompliance firstKey BottleneckCredentialing gateProvider coverageFirst Revenue StepBooked consultsBilling live
Launch timeline
Short web summary of the launch plan; the XLSX export contains the detailed Gantt chart.
What licenses do you need to open a psoriasis treatment center?
To open a Psoriasis Treatment Center, you need licensed clinical providers, a compliant medical entity, required clinic registrations, prescribing authority, HIPAA and OSHA readiness, malpractice coverage, and payer enrollment before patients are treated or billed; use How To Write A Business Plan For Psoriasis Treatment Center? to map these steps into your launch plan. This is compliance guidance, not legal advice, and state medical board rules matter because psoriasis affects over 7.5 million U.S. adults and treatment can involve prescriptions, phototherapy, biologics, records, claims, and supervision.
Core licenses
Verify state medical board rules
Confirm corporate practice limits
Register the clinic if required
Check prescribing and supervision authority
Launch order
Set ownership and licensure first
Secure lease, hiring, and credentialing
Implement EMR, HIPAA, and billing
Budget for OSHA penalties up to $165,514
How long does it take to open a psoriasis clinic?
A Psoriasis Treatment Center usually takes 6–12 months to open. The pace depends on provider recruiting, payer credentialing, facility buildout, phototherapy equipment delivery, EMR setup, billing workflows, and referral pipeline readiness. Start payer work once providers and tax details are set, and don’t wait for construction to build referral ties.
Main timing drivers
6–12 months is the practical range
Dermatologist availability can slow launch
Insurer enrollment often bottlenecks
Equipment and EMR setup take time
What “open” means
Schedule consults and follow-ups
Run phototherapy visits if offered
Submit clean claims to payers
Keep referral flow active early
How do you get patients for a psoriasis treatment center?
Fill a Psoriasis Treatment Center by building referrals from dermatologists, primary care physicians, and rheumatologists, plus local search and insurer directories. For launch steps, see How Do I Launch Psoriasis Treatment Center?; the first revenue usually comes from consults, follow-ups, phototherapy visits, and insured treatment plans.
Referral setup
Build ties with 3 referral groups.
Set up insurer directory listings.
Post psoriasis condition pages.
Share education content with care networks.
Convert visits
Promote phototherapy availability clearly.
Book follow-ups before patients leave.
Track booked consults and show rates.
Watch referral source and inquiry-to-visit time.
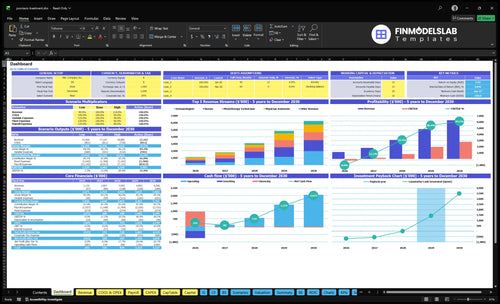
Psoriasis Treatment Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before seeing psoriasis patients
Launch readiness checklist
Use this go-live approval checklist to confirm the psoriasis treatment center is ready before opening.
1Compliance
State compliance reviewedCritical
Confirm state rules, clinic registration, HIPAA, and OSHA before patient care starts.
Ownership structure approvedCritical
The entity and owners must match state rules before contracts and payroll start.
Provider licenses activeCritical
Every dermatologist, PA, and nurse needs an active license before care.
Prescribing authority verifiedCritical
Use documented scope rules for psoriasis meds before treatment starts.
Malpractice coverage boundCritical
Claims start on day one, so coverage must be active at opening.
2Facility
Treatment rooms readyHigh
Room count and layout must support exam, treatment, and follow-up visits.
ADA access clearedHigh
Patients must enter, move, and exit safely with ADA access in place.
Infection control readyCritical
Hand hygiene, cleaning, and waste flow must be set before the first visit.
Refrigerated storage installedHigh
Biologics need secure cold storage before medication inventory arrives.
3Equipment
Phototherapy units installedCritical
Units must be installed and tested before the first light treatment.
EMR configuredCritical
Notes, meds, photos, and follow-up templates must work on day one.
Equipment maintenance plannedHigh
A service plan reduces downtime for core devices after launch.
Diagnostic tools readyHigh
Exam and biopsy tools must be ready for first patient workups.
4Staffing
Care team staffedCritical
Coverage must match the Year 1 plan so visits do not stall.
Provider schedules postedHigh
Open slots need to match demand and the phototherapy calendar.
Psoriasis training completedCritical
Staff should know treatment paths, side effects, and escalation steps.
Escalation coverage setHigh
Backups must be named for absences, urgent calls, and refill issues.
5Revenue flow
Billing codes loadedCritical
Charge capture must fit psoriasis visits, procedures, and follow-ups.
Payer enrollments activeCritical
Claims cannot move until payer links are active.
Prior authorization workflow testedCritical
Biologics often need approval, so test the full path before launch.
Insurer directory updatedHigh
Patients need correct listings so they can find and reach the clinic.
Referral and specialty contacts setHigh
Referrers and specialty pharmacies must know who handles each case.
6Finance
Cash runway confirmedCritical
The model hits a $230k cash floor in Month 13, so funding must survive the dip.
Opening forecast approvedHigh
Breakeven is Month 14, so the opening plan must support the ramp.
Go-live signoff completeCritical
No launch until compliance, staffing, EMR, and billing owners sign off.
Want to review the main psoriasis clinic launch drivers?
1Compliance Structure
License gate
Compliance must clear first, or patient intake, billing, and marketing all slide back.
2Provider Staffing
1 Derm
One dermatologist, one physician assistant, two nurses, and one phototherapy tech set day-one capacity.
3Payer Credentialing
Claims live
Active payer contracts stop the common trap: patients in, cash delayed.
4Facility And Equipment Readiness
45% cap
Installed phototherapy and exam-room gear cut cancellations and keep opening on schedule.
5Clinical And Billing Workflows
$1.2K/mo
The $1.2K EMR setup must work before volume ramps, or cash conversion slows.
6Patient Acquisition
$94K/mo
Referral and search setup fill the calendar before payroll starts and support early recurring care.
Compliance Structure
Compliance Structure
For a psoriasis treatment center, compliance is the gate before patient care and marketing. Do not open until state-specific ownership structure, provider licensure, malpractice coverage, HIPAA, OSHA, prescribing authority, and clinic registration where required are cleared. If this slips, the fix usually shows up as rework after lease signing, which can push back launch.
One clean rule: if the medical structure is not legally ready, the clinic is not ready to see patients. That delay hits credentialing, billing, and patient intake at the same time, so day-one operations start behind schedule instead of on plan.
Lock Compliance First
Start with healthcare counsel review and medical board verification. Then set up the entity so it is payer-ready, and finish privacy training, safety policies, and documentation standards before you commit to the space. That order keeps the launch plan tied to what you can legally operate, not just what you can lease.
Confirm ownership rules first.
Verify licensure and prescribing authority.
Set malpractice and HIPAA coverage.
Train staff on privacy and safety.
Register the clinic where required.
What this avoids is simple: a signed lease with a clinic that cannot bill, prescribe, or open cleanly. When compliance is done up front, credentialing, billing, and patient intake can start with fewer delays and less cash strain on opening day.
1
Provider Staffing
Provider Staffing
A psoriasis clinic can’t open on time without the right prescribers and support team. The dermatologist is the key gatekeeper because they drive prescribing authority, supervision for the physician assistant, payer enrollment, and clinical credibility on day one.
The Year 1 plan assumes 1 dermatologist, 1 physician assistant, 2 nurses, 1 phototherapy technician, and 1 medical assistant, plus operations roles. If hiring slips, consult slots, treatment coverage, and photo therapy hours all shrink, so the first revenue ramp gets slower and the schedule gets harder to run cleanly.
Build the roster before the calendar
Start with the hiring sequence, then lock the operating setup. The readiness signal is signed schedules, supervision rules, credentialing packets, and treatment coverage. Here’s the quick check: recruiting, onboarding, payer enrollment, clinical protocols, and calendar buildout all need to line up before the first patient slot is sold.
Hire the dermatologist first.
Confirm PA supervision rules.
Finish credentialing before opening.
Test treatment coverage by shift.
Build the schedule around capacity.
What this plan hides is timing risk. If the dermatologist comes in late, the clinic may still have staff on paper, but it won’t have full prescribing authority or stable coverage. That can push back first consults, create schedule gaps, and slow day-one revenue even if the lease and equipment are ready.
2
Payer Credentialing
Payer Credentialing
For a psoriasis clinic, payer credentialing is the gate between opening on time and getting paid. Psoriasis care often includes recurring visits, specialty medications, covered procedures, and prior authorization, so the clinic needs active payer contracts, loaded fee schedules, billing rules, and claim workflows before it can run cleanly from day one.
Here’s the quick math: if patients are booked before enrollment is live, the clinic can still deliver care, but collections lag. That creates a cash gap right when staffing, billing, and software costs start. What this hides is simple: you can open the doors, but delayed payer setup can turn first revenue into slow, uncertain reimbursement.
Credential Before First Visits
Set up payer work in a strict order: provider enrollment, clearinghouse setup, coding review, denial workflow, specialty pharmacy coordination, and benefits verification. Each step protects first-week cash flow because psoriasis treatment plans can trigger claim edits, prior auth holds, and follow-up billing issues. Assign one owner to each payer, form, and deadline.
Before opening, verify active payer contracts, loaded fee schedules, and a tested path from chart to claim submission. Also test prior authorization tracking so consults, follow-ups, and treatment plans do not stall after the visit. If the clinic can bill cleanly in week one, collections start steadier instead of lumpy.
Confirm each payer’s enrollment status
Load fee schedules before booking
Test claims and denial routing
Set prior auth owners and alerts
Coordinate specialty pharmacy handoffs
3
Facility And Equipment Readiness
Facility Readiness
Facility readiness is what lets the clinic open on time and safely treat patients on day one. If the exam rooms, treatment rooms, ADA access, infection control, storage, and safe phototherapy workflow are not ready, the opening date slips even if hiring and billing are done.
Here’s the quick math: Year 1 assumes 1 phototherapy technician and 200 monthly phototherapy treatment capacity. At the 45% utilization assumption, that’s about 90 treatments per month. That only works if equipment is installed, staff are trained, and maintenance is scheduled before the first visit.
Lock the Buildout Early
Verify equipment purchase or lease dates against buildout timing, inspections, and move-in. Confirm the room layout supports patient flow, storage, and treatment safety before you sign off on the space. If the layout is wrong, you can be “open” on paper but still cancel visits in practice.
Match delivery dates to lease start.
Test phototherapy workflow before opening.
Train staff on safety procedures.
Document maintenance and cleaning steps.
Late equipment delivery or a buildout mismatch is the main bottleneck here. That usually means fewer cancellations only after the room is ready, so the opening plan needs a clear install schedule and a signed readiness checklist.
4
Clinical And Billing Workflows
Day-One Billing Flow
For a psoriasis treatment center, this driver decides whether the clinic can see patients and get paid on day one. Scheduling, intake, documentation, coding, claims submission, prior authorization tracking, treatment protocols, lab coordination, and specialty pharmacy communication all have to work together, or visits pile up and cash gets stuck. The fixed EMR cost of $1,200 per month only makes sense if the workflow is live before volume starts.
The readiness signal is a tested EMR and billing setup with clean superbills, benefits checks, follow-up templates, and one person owning denials. If that is weak, the clinic can still open, but unpaid claims and missed follow-ups will slow early revenue and create avoidable rework. One clean first week matters more than a busy calendar.
Test the Full Revenue Path
Before opening, run one sample patient from check-in to claim close. Verify the EMR, coding rules, prior authorization steps, lab handoffs, and specialty pharmacy messages. Make sure every note maps to a superbill and every denial has an owner. That turns the launch from theory into a working process.
Load follow-up templates before first visit.
Confirm benefits checks on day one.
Assign denial ownership in advance.
Test claims before patient volume rises.
If the workflow breaks, fix it before the schedule fills. Early delays here hit both patient experience and cash conversion fast.
5
Patient Acquisition
Patient Demand
Opening days live or die on booked consults. For a psoriasis clinic, patient acquisition is not just ads; it’s referral relationships, insurer directory visibility, local search setup, psoriasis condition pages, education content, and follow-up conversion. If those pieces are not live before payroll starts, the main risk is an empty schedule from day one.
Year 1 marketing and patient acquisition is modeled at 30% of variable expense, so every $100 of revenue needs $30 to keep demand coming in. By Year 5, that falls to 22%, but only if the clinic can turn searches and referrals into booked consults, phototherapy visits, and recurring care plans.
Fill Before Open
Before launch, verify live profiles, referral scripts, and an outreach list with named sources. Publish the psoriasis condition pages and education content early, then connect every lead source to appointment tracking so you can see what fills slots, not just what gets clicks.
Confirm insurer directory accuracy
Test referral outreach scripts
Track consults by source
Review claims language for compliance
Also test follow-up conversion before opening. If a booked consult does not turn into a treatment plan or return visit, the schedule can look healthy on paper while cash stays thin. That is the launch risk this driver is meant to control.
Start by defining the clinical scope before signing a lease Decide whether opening month includes consults only, consults plus follow-ups, or phototherapy too The base Year 1 model assumes 1 dermatologist, 1 physician assistant, 2 nurses, 1 phototherapy technician, and 1 medical assistant at 45% capacity
Plan the payer work inside the 6–12 month launch window Billing readiness needs provider enrollment, payer contracts, coding setup, EMR workflows, benefits checks, and prior authorization tracking If contracts are not active by opening month, you may see patients but delay collections, which strains cash
No, but the answer depends on your launch scope A lean clinic can start with consults, follow-ups, and medication management, then add phototherapy later The base model includes 1 phototherapy technician in Year 1, with 200 monthly treatment capacity before applying the 45% utilization assumption
The base Year 1 staffing plan includes 1 dermatologist, 1 physician assistant, 2 nurses, 1 phototherapy technician, 1 medical assistant, 1 practice manager, 05 billing specialist, and 1 receptionist That structure supports consults, clinical care, treatment visits, scheduling, billing, and patient follow-up
Confirm the compliant operating structure and provider plan first State medical rules, ownership limits, provider licensure, malpractice coverage, and payer enrollment requirements can shape the lease, room count, and launch date If the space cannot support treatment rooms, patient flow, and equipment needs, the buildout can slow opening
About the author
Nathan Ellis
Independent Business Researcher
Nathan Ellis is an independent business researcher who writes practical guides for people planning their first business. He focuses on small business money management, helping online business beginners turn business assumptions into a clear plan. His work uses simple revenue and profit examples and explains business costs without unnecessary jargon, keeping the numbers realistic and easy to follow.
Choosing a selection results in a full page refresh.