How to Open a Drug and Alcohol Rehab Center in 6 to 12+ Months
To open a drug and alcohol rehab center, define the care model first, then confirm state licensing, secure a compliant site, write clinical policies, hire credentialed staff, and test admissions before accepting clients A practical planning range is 6 to 12+ months, but timing varies by state, care level, zoning, accreditation, payer contracts, and buildout In the Year 1 model, ramp assumptions start at 40% detox capacity, 35% residential capacity, and 30% individual therapy capacity, so first revenue depends on clinically appropriate intakes, not full occupancy on day one
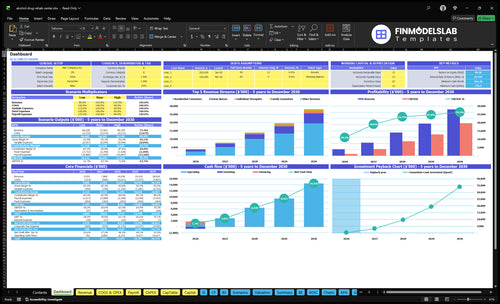
Time to Open6 monthsOpening prepLaunch Sequence5 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepFirst intakeIntake ready
Launch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt Chart.
A Drug and Alcohol Rehab Center needs state substance use treatment licensure first; there is no single national license that lets you open everywhere. Match the care model before filing because residential care, outpatient therapy, detox, and medication-assisted treatment, or MAT, can trigger different approvals; review What Is The Current Growth Trajectory Of Your Drug And Alcohol Rehab Center? while tying license timing to launch risk. The model carries $1,000/month for licensing and accreditation, but the bigger risk is delayed approval in a market where 48.5 million US people aged 12+ had a substance use disorder in 2023.
Core licenses
Get state substance use treatment approval
Match residential, outpatient, detox categories
Add MAT and controlled-substance approvals
Secure facility, zoning, and occupancy clearance
Opening risks
Budget $1,000/month for approvals
Plan inspections before client intake
Meet staffing and documentation rules
Add payer and accreditation requirements early
How long does it take to open a rehab center?
A Drug and Alcohol Rehab Center usually takes 6 to 12+ months to open, and residential or detox sites often run longer than outpatient ones because licensing, zoning, occupancy, life-safety checks, staffing, and payer setup all have to line up. If the lease starts before approval, the math gets ugly fast: a $25,000 monthly facility lease plus $37,800 in fixed overhead can burn cash before the first admission. The real risk is sequence, not the average date.
What drives timing
State licensing review sets the pace.
Zoning and occupancy can delay launch.
Life-safety inspections must pass first.
Clinical hiring and policy approval take time.
Why sequence matters
Lease-first setups can burn cash early.
$25,000 rent starts before admissions revenue.
$37,800 fixed overhead compounds the risk.
Residential and detox models need more site work.
How do rehab centers get clients?
A Drug and Alcohol Rehab Center gets clients through ethical referrals, online search, and community outreach, not pressure or shortcuts. The first gate is intake: clinical screening, fit review, insurance check, and bed or schedule availability; for setup context, see What Is The Estimated Cost To Open A Drug And Alcohol Rehab Center?. Year 1 usually ramps in partial capacity, with only 40% detox, 35% residential, 30% individual therapy, 25% family counseling, and 40% physician visits filled at first.
Client sources
Hospitals and discharge planners refer.
Therapists and physicians send patients.
Courts refer only when appropriate.
Employee Assistance Programs and alumni help.
Admissions filter
Screen first for clinical fit.
Verify insurance before admission.
Match care to available beds.
Follow up fast after contact.
Key Takeaways
Licensing approval sets the legal launch date.
Facility clearance must come before hiring and marketing.
Clinical policies and credentials drive safe daily operations.
Payer setup must work before first intake.
State Licensing Path
State License First
State licensing is the first hard gate. It sets the care level, opening date, staffing rules, documentation, inspection steps, and whether you can legally start services. If you pick the wrong category, like residential, outpatient, detox, or medication-assisted treatment, you can delay launch or force a redesign after the lease is signed.
Do not market beds, hire to full capacity, or lock in a site until the state confirms the intended service mix. The readiness signal is simple: written approval or certification for the exact scope you plan to open with.
Map Scope Before Spend
Start with the license category, then map the service mix, policies, and inspection items. Build the application packet around required documents, facility standards, and staffing rules, then track each gap to closure. One clean file beats a rushed launch.
Confirm state license category
Match scope to services
Prepare policies and forms
Track inspection punch list
Wait for written approval
If the license path slips, opening slips with it. That can leave you paying rent, carrying payroll risk, and holding empty beds while revenue stays at zero.
1
Compliant Facility Readiness
Facility Readiness
If the site cannot clear zoning, the certificate of occupancy (city approval to use the building), life-safety, and accessibility checks, the center cannot open on time. Residential and detox layouts are tighter than outpatient, so bedroom count, therapy rooms, privacy, and medication storage have to match the licensed care level before staff arrive and the first client is scheduled.
This is also a cash issue. The lease is $25,000/month and fixed overhead is $37,800/month before wages, so a delayed inspection or bad layout keeps money burning while no one can be served. The readiness signal is a site that passes state, local, fire, safety, and occupancy review with no open items.
Lock the site plan early
Start with a room-by-room checklist tied to the care model, then get zoning and occupancy confirmed before you sign or finish buildout. One clean line: no approval, no opening.
Confirm allowed use and zoning.
Book life-safety inspection early.
Document accessibility and privacy.
Set medication storage and controls.
Match rooms to licensed care level.
Track each permit, inspection, and correction on one launch sheet. If the site needs rework after furniture, signage, or med storage is installed, opening slips and day-one operations start with avoidable gaps.
2
Clinical Program And Policies
Clinical Program Design
This driver turns the license into daily care. Before opening, the team has to define levels of care, admissions criteria, assessment workflow, and medical escalation steps for detox, residential counseling, individual therapy, family counseling, and physician visits. If those rules are vague, staff slow admissions, miss handoffs, or make unsafe calls, and the opening slips because policies fail review.
The real readiness test is a signed clinical operations manual that staff can use during mock admissions. It should cover treatment plans, group programming, discharge planning, crisis response, and documentation standards. One clean rule: if a nurse, counselor, and physician all read it the same way, you are closer to opening on time.
Test the Manual Before Intake
Map the intake path in the order staff will use it: screening, assessment, placement, treatment plan, and charting. Tie each step to one owner and one form, so the process works before census starts. This is where launch risk sits—unclear policy language can stall approvals, confuse new hires, and create uneven care on day one.
Before opening, run a fake admission across every service line in scope. Use detox, counseling, family sessions, and physician review to check timing, notes, and escalation. If the team cannot complete the scenario without rework, the program is not ready for live clients yet.
3
Credentialed Staffing
Credentialed Staffing
Staffing is what turns the license into real care. Headcount has to match license type, census capacity, acuity, and service mix, or the center cannot open with safe day-one coverage. The Year 1 model assumes 3 detox nurses, 5 residential counselors, 4 individual therapists, 2 family counselors, 1 medical doctor, and a clinical director paid $120,000 per year.
Delay the roles tied to licensure, and the opening date slips fast. That can leave a ready site idle while fixed overhead still runs at $37,800 per month before wages. One missing credential can stall the whole launch.
Verify licenses before you schedule intake
Build the roster from the care plan, then verify every credential before move-in. Confirm the clinical director, licensed counselors, nurses, and the medical doctor if your license requires one. Add case managers, admissions staff, and compliance leadership early so intake, charting, and oversight work from day one.
Check each license and expiration date.
Match shifts to care level.
Document supervision and backup coverage.
Test coverage before first admission.
The readiness signal is simple: credential verification, shift coverage, supervision plan, and backup coverage. If any of those are weak, you risk missed assessments, unsafe handoffs, and a launch that opens late but still burns cash.
4
Admissions And Referral Pipeline
Admissions Pipeline
Admissions has to be live before opening month, or the center opens with empty beds and a slow first census. This work covers referral outreach, intake screening, clinical fit review, insurance verification, call handling, follow-up cadence, and real-time bed or schedule checks, so the team can accept the right clients on day one.
The launch risk is simple: if scripts, criteria, and tracking are not tested, leads get lost, unsuitable admits slip through, and staff time gets wasted. Year 1 utilization is modeled at 25% to 40% depending on service line, so the intake funnel has to be ready before the first client walks in.
Test Intake Before Open
Build the pipeline around documented admission criteria, a live referral list, and a clear follow-up schedule. Sources can include hospitals, therapists, physicians, courts where appropriate, employee assistance programs, alumni, online search, and community outreach, but each source needs a tracked owner and response time.
Run mock calls before opening and verify three things: clinical fit, insurance status, and bed or schedule availability. If the center cannot answer, screen, and book in one pass, first-day occupancy will lag even if demand is there.
Test intake scripts with real scenarios.
Document exclusion and acceptance rules.
Track every referral source weekly.
Set follow-up timing before launch.
Match admits to open capacity only.
5
Payer And Revenue-Cycle Readiness
Payer And Billing Setup
Payer contracting and revenue-cycle setup decide when admissions turn into cash. A rehab center can’t treat billing as back office work; it affects opening date, first-day operations, and whether early census creates real cash or just paper revenue.
The setup includes the private pay, in-network, or out-of-network path, plus insurance verification, utilization review, documentation rules, billing codes, claims filing, and denial tracking. If benefits and payer rules aren’t verified before first intake, the center can open with demand but still face slow collections and avoidable cash strain.
Build Cash Collection Before Intake
Set the billing flow before the first admission. Verify benefits, map payer rules, load the right billing codes, and train staff on documentation standards so clinical notes support claims from day one. The readiness signal is simple: verified benefits, a live claims process, and a clear cash collection path before any intake is booked.
Test insurance verification before opening.
Assign ownership for denials daily.
Train staff on note timing.
Review payer timing against $326,600 monthly revenue.
Flag any collections lag early.
Here’s the quick math: if Year 1 monthly revenue is about $326,600 at stated utilization, delayed reimbursement can create a gap between service delivery and cash receipt. That gap matters most in month one, when payroll, vendors, and facility costs start on time but collections may not.