How To Open An Allergy And Immunology Clinic In 4–9 Months
Opening an allergy clinic takes about 4–9 months in most launch plans because payer credentialing, lease/buildout, staffing, EHR setup, malpractice coverage, and clinical workflows must run before the first patient day The core steps are entity setup, physician readiness, location, payer enrollment, clinical setup, staff hiring, referral outreach, and soft launch In the Year 1 model, one allergist, one nurse practitioner, and one allergy nurse support about $75,000/month in modeled revenue at stated capacity The bottleneck is usually payer enrollment plus safe testing and immunotherapy readiness
Time to Open4-9 monthsSetup windowLaunch Sequence8 stagesCompliance firstKey BottleneckCredentialing gateApproval pathFirst Revenue StepBooked consultsBooking live
Launch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt chart.
Confirm what must be ready before first patient day
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
1Compliance
Entity registration filedCritical
The clinic needs a legal entity before contracts, banking, and payer setup start.
State licenses activeCritical
Provider licenses must be active before any patient care begins.
NPI numbers issuedCritical
The NPI is needed for claims, referrals, and payer enrollment.
Malpractice policy boundCritical
Coverage should be bound before the first visit or procedure.
2Site
Lease signed and liveCritical
The clinic site must be secured before buildout and move-in costs hit.
Buildout passed inspectionCritical
Rooms, sinks, storage, and patient flow need to be ready for safe use.
HIPAA safeguards enabledCritical
Patient data must be protected before records and scheduling go live.
OSHA basics documentedHigh
Safety rules reduce injury risk and support staff compliance from day one.
3Clinical systems
EHR workflow testedCritical
The EHR must support notes, orders, and follow-up without workarounds.
Billing codes loadedHigh
Clean coding helps claims move fast and cuts rejected payments.
Consent forms approvedHigh
Allergy testing and immunotherapy need the right consent before care starts.
Referral intake routedMedium
Referral flow should send new patients to the right visit type fast.
4Supplies
Allergy test kits stockedCritical
Testing cannot start without enough kits for the first patient schedule.
Immunotherapy storage validatedCritical
Vials need stable storage so treatments stay safe and usable.
Emergency medications on handCritical
Emergency meds must be ready before any allergy injection or test.
Cold chain logs readyHigh
Temperature logs prove storage stayed in range for immunotherapy products.
5Staffing
Physician coverage assignedCritical
A physician must be assigned to supervise clinical care and escalation.
Nurse schedules postedHigh
Staff schedules need to cover intake, testing, treatment, and follow-up.
Training completed for protocolsCritical
Staff must know testing, injection, reaction, and documentation steps.
Escalation roles confirmedCritical
Everyone needs a clear backup path when a patient reacts or needs help.
6Revenue
Online scheduling liveHigh
Patients need a working way to book the first visit without a phone delay.
First referrals outreach sentHigh
Referral outreach helps fill the first schedule and build early demand.
Billing workflow readyCritical
The clinic must be able to document, code, submit, and track claims.
Cash runway covers Month 5Critical
Minimum cash hits in Month 5, so funding must carry the early burn.
Want the six launch drivers that decide go-live readiness?
1Payer Credentialing
Claim gate
Active payer contracts or a self-pay policy are the gate to booking insured visits and clean claims.
2Facility Ready
4-9 mo
A ready space for consults, testing, refrigeration, and emergency response cuts day-one safety and workflow failures.
3Staff Hiring
3 key hires
Year 1 coverage needs 1 allergist, 1 nurse practitioner, and 1 allergy nurse to keep consults and follow-up moving.
4Testing Workflow
400/mo
Documented testing, storage, consent, and observation steps convert consults into treatments without day-one bottlenecks.
5EHR & Billing
3% fees
Tested scheduling, charting, and claims flow protect reimbursement and prevent documentation gaps at go-live.
6Referrals
4% rev
Local outreach and online scheduling drive consults, testing visits, and follow-up once the doors open.
Why test the Allergy and Immunology Clinic model before launch?
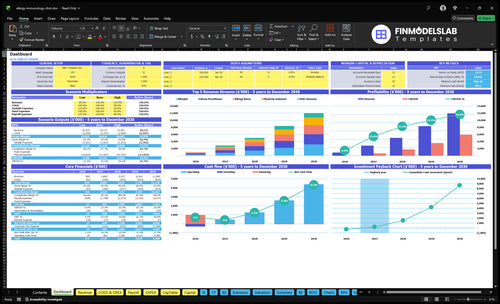
The screenshot shows the dashboard, revenue ramp, staffing tab, assumptions table, and charts to test payer mix, patient ramp, testing volume, immunotherapy visits, runway, and breakeven; open the Allergy and Immunology Clinic Financial Model Template.
Financial model highlights
1 allergist, 1 NP
65% to 75% capacity
$75,000 monthly revenue
4% supplies cost
5% vials cost
3% billing fees
4% marketing spend
How long does payer credentialing take for an allergy clinic?
Payer credentialing for an Allergy and Immunology Clinic should start on day one and run beside lease, buildout, and hiring, because it sits inside the usual 4–9 month launch window. The file needs to be clean: provider documents, malpractice coverage, National Provider Identifier (NPI), CAQH profile, tax ID, practice address, payer applications, EHR setup, billing workflows, and eligibility checks. If any piece is missing, or if permits, supplies, or allergy testing workflows are not ready, opening slips.
Start early
Day-one task, not later.
Run with buildout and hiring.
Use complete provider files.
Keep NPI and CAQH ready.
Common delay points
Incomplete payer files slow approval.
Permits can delay the opening date.
Untested billing breaks first claims.
Missing supplies and workflows add risk.
How does a new allergy clinic get patients?
A new Allergy and Immunology Clinic usually gets its first patients from primary care, pediatrician, and ENT referrals, plus local search, accepted-insurance listings, and online booking. For the cost side, see How Much Does It Cost To Open An Allergy And Immunology Clinic? First revenue usually comes from consults, allergy testing, and follow-up treatment plans, and the Year 1 model supports about $75,000/month at stated capacity. Keep outreach referral-focused and compliant, with 4% of revenue set aside for marketing and patient acquisition.
Patient sources
Primary care sends early referrals
Pediatricians drive child allergy cases
ENT physicians add specialty referrals
Search and insurance listings bring intake
Revenue drivers
Consults open the first visits
Testing lifts early billings
Follow-ups build repeat revenue
Online scheduling speeds conversion
What launch mistakes delay an allergy practice opening?
For the Allergy and Immunology Clinic, the biggest launch mistake is opening before payer contracts, EHR templates, billing workflows, emergency protocols, and immunotherapy handling are ready. With millions of Americans needing allergy care, a rushed soft launch can still miss revenue if the clinic can’t verify eligibility, submit clean claims, store extracts, document observation, or schedule follow-ups. Use a go/no-go checklist before soft launch so safe care, clean billing, and first-revenue conversion start together.
Launch blockers
Payer contracts not active yet
EHR templates still incomplete
Billing rules not tested
Emergency steps not trained
Readiness checks
Immunotherapy storage and handling set
Staff trained on protocols
Referrals and outreach ready
Scheduling and follow-ups mapped
Key Takeaways
Credentialing first, or insured billing stalls at launch.
Facility readiness prevents day-one safety and workflow problems.
Staffing coverage protects consults, testing, and follow-up.
Systems and referrals drive cleaner revenue capture.
Payer Credentialing
Payer Credentialing
If insured patients will be seen on Day 1, payer credentialing is the gate. The clinic cannot reliably schedule or bill those visits until contracts are active, or it has a clear self-pay policy before booking. Without that, you get a soft opening with no clean claim path, and cash starts slipping.
The file set is specific: provider documents, malpractice coverage, National Provider Identifier (NPI), CAQH, tax ID, location details, payer applications, and billing setup. If one piece is missing, consults and testing may still happen, but first revenue gets delayed because the visit can’t be billed cleanly.
Credential Before You Book
Start credentialing before you market insured appointments. The readiness signal is simple: active contracts in hand, or a written self-pay script for every visit type. That keeps front desk, billing, and scheduling aligned from Day 1.
Submit provider and malpractice documents.
Finish NPI, CAQH, and tax ID.
Load every clinic location.
Test claims before opening.
Set self-pay pricing in writing.
What this hides: if credentialing runs late, staff may be ready but revenue is not. That raises cash needs, forces awkward scheduling decisions, and can slow the handoff from consults to testing and billed care.
1
Clinical Facility And Equipment Readiness
Facility Ready to Open
An allergy clinic can’t open on time if the space does not fit the services. The room plan has to support consults, skin testing, spirometry or breathing checks, immunotherapy prep, refrigeration, emergency response, patient flow, and an accessible front desk.
The real risk is a day-one scramble. If the lease, buildout, or equipment setup slips, staff end up working around the space instead of using it. That raises safety risk, slows visits, and can force a soft opening with fewer clean patient encounters from day one.
Preopen Setup Checks
Match the layout to the services you will actually offer and the state rules that apply. Before opening, verify room use, storage logs, refrigeration, emergency access, and how patients move from check-in to testing to follow-up. If any step is missing, fix it before scheduling the first patient.
Confirm lease and buildout timing.
Assign rooms for consults and testing.
Set up refrigeration and logs.
Test emergency and patient flow paths.
Check front desk accessibility.
Do the equipment walk-through before launch, not after. The clinic should be able to receive deliveries, place equipment, and run a basic patient flow test without rework, because a space that looks finished but fails setup still delays opening and burns cash on rent and labor.
2
Physician And Staff Hiring
Day-One Clinical Coverage
An allergy clinic can’t open safely if the allergist or qualified provider, 1 nurse practitioner, and 1 allergy nurse are not trained and scheduled for consults, testing, documentation, claims, and follow-up. That Year 1 staffing shape is the readiness check. If one role is missing, you risk a soft open, lower capacity, or a launch delay.
This plan also has to cover front desk, scheduling, billing, prior authorizations, and biologic or immunotherapy coordination. If those handoffs are weak, day-one patients wait longer, claims sit unfiled, and the clinic feels disorganized even if the rooms are ready. One weak link can slow the whole first month.
Train the Full Patient Flow
Before opening, assign each person’s first-week job in writing and cross-train the team on the full visit path. The key test is simple: can one patient move from scheduling to consult, testing, documentation, claim submission, and follow-up without the founder stepping in every time?
Use a short launch checklist with coverage for consults, testing support, prior authorization handling, and immunotherapy coordination. If any step depends on one untrained person, the launch is fragile and first-revenue timing slips.
Confirm provider coverage by opening day.
Train on consults, claims, and follow-up.
Assign one owner for prior authorizations.
Test biologic and immunotherapy handoffs.
3
Allergy Testing And Immunotherapy Workflow
Testing And Immunotherapy Flow
Allergy testing and immunotherapy flow has to work before the first day. If documented protocols, extract suppliers, storage logs, patient consent, emergency medications, observation workflow, charting templates, and follow-up scheduling are not in place, consults turn into delays instead of treatment starts. That is a launch risk, not a clinical theory problem.
The bottleneck shows up fast once consults convert into testing and treatment plans. If one step fails, nurses wait, rooms sit idle, and patients get pushed out, which hurts first-day revenue and trust. One missing log can stop the day.
Day-One Flow Check
Before opening, run one patient from consult to follow-up on paper and in the EHR to confirm every handoff works. The readiness signal is simple: the protocol binder, supplier list, storage log, consent form, emergency kit check, observation timer, charting template, and follow-up slot all close without a gap.
Verify extract lead times.
Assign storage log ownership.
Test consent at intake.
Stage emergency meds access.
Template observation and follow-up notes.
Here’s the quick math: 400 monthly treatments at $75 each is $30,000 in treatment revenue. At 75% capacity, that is 300 treatments and about $22,500 monthly, so workflow gaps delay real cash, not just scheduling.
4
EHR Billing And Compliance Systems
EHR and Billing Workflow
Your clinic cannot open cleanly if scheduling, charting, eligibility, and claims do not work together. For an allergy practice, the readiness test is simple: one patient must move from appointment to chart note to claim submission without gaps. If that loop is weak, you can still see patients, but you risk delayed cash, denied claims, and messy follow-up on day one.
This launch driver includes intake forms, prior authorization handling, HIPAA safeguards, OSHA basics, and reporting. Year 1 billing service fees are modeled at 3% of revenue, so the system has to be live before the first visits. Clean documentation is the bottleneck; without it, reimbursement slows and first-day revenue leaks.
Test the full claim path
Before opening, test one full visit end to end: scheduling, intake, eligibility, charting, prior auth, claim scrub, and same-day claim submission. The owner should assign who fixes failed fields, who checks payer rules, and who sends claims. That keeps day-one cash flow realistic.
Match intake forms to chart fields.
Run one test claim to submission.
Document prior auth and eligibility steps.
Set access controls for HIPAA and OSHA.
Check reporting before the first patient.
A weak launch here means patients are seen before the back office can bill, and that turns clinical work into unpaid work.
5
Referral And Patient Acquisition Engine
Local Referral Engine
A local referral engine decides whether the clinic opens with real patient flow or an empty schedule. Local search visibility, accepted insurance visibility, and referral paths from primary care, pediatrics, and ear, nose, and throat offices need to be live before opening so consults, testing visits, and follow-up plans can start on day one.
Year 1 marketing and patient acquisition is modeled at 4% of revenue, so this is a controlled setup cost, not a volume promise. If online scheduling, review handling, or referral outreach is late, the clinic can still open, but first-revenue timing slips because patients and referring offices have nowhere clean to send them.
Pre-Opening Referral Checklist
Build the patient path before the doors open. Keep online scheduling, insurance display, and local search profiles active, then confirm outreach to primary care, pediatrics, and ear, nose, and throat practices. The goal is simple: every channel should point to a bookable visit, not just awareness.
Verify search listings are live.
Show accepted insurance clearly.
Test online booking end to end.
Document referral contact names.
Run a review request process.
Model Year 1 spend at 4% of revenue and do not promise patient volume. If the intake handoff is slow or confusing, opening day still happens, but consults, testing visits, and follow-up plans will convert more slowly.