How To Open A Behavioral Health Center: 6–12+ Month Launch Roadmap
You’re opening a care business where licensing, staffing, payer setup, and referral readiness must line up before the first intake This launch plan covers a 6 to 12+ month opening path and a Year 1 operating model with 7 clinicians and about $85,140/month in modeled capacity revenue Start by validating your service mix, approvals, EHR, billing workflow, and first referral sources before signing up clients
Time to Open9 monthsLaunch runwayLaunch Sequence7 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepPaid evalIntake ready
Launch timeline
This short web summary shows the launch path; the XLSX export holds the detailed Gantt chart.
What licenses are needed to open a behavioral health center?
A Behavioral Health Center usually needs entity formation, state behavioral health or healthcare facility approval, local zoning clearance, clinical leader approval, staff license checks, privacy workflows, written policies, and emergency procedures. Requirements vary by state, service line, and payer, so verify rules before lease or launch commitments; track licensing beside What Is The Most Critical Metric To Measure The Success Of Your Behavioral Health Center?.
Core approvals
Form the legal entity
Clear local zoning review
Secure state facility approval
Verify every clinician license
Extra checks
Substance use care may add rules
Medication management may trigger oversight
Medicaid and insurers add credentialing
NIMH 2022: 59.3M adults affected
How do you get clients for a behavioral health center?
Get clients before you open: build intake-ready referrals from primary care physicians, hospitals, therapists, schools, employers, community organizations, employee assistance programs, courts where appropriate, and local search. With Year 1 modeled capacity at about 592 visits per month, your outreach should match payer acceptance and service scope so every referral can turn into a scheduled assessment. See How Much Does It Cost To Open A Behavioral Health Center? for the setup side.
Build referral sources first
Target primary care doctors
Ask hospitals for discharge referrals
Work with therapists and schools
Use employers and EAPs
Match outreach to capacity
Fill 592 monthly visits first
Promote only staffed services
Keep claims aligned with compliance
Push scheduled assessments early
How long does it take to open a behavioral health center?
A Behavioral Health Center usually takes 6 to 12+ months to open, and the lease is rarely the main delay. The real bottlenecks are the approval chain: state licensing review, facility inspections, payer credentialing, clinical hiring, EHR implementation, and fixing incomplete policies before launch. Start payer and clinician credential files as soon as the service model is set, and don’t set a hard opening date until license status, clinical coverage, intake documentation, claims workflow, and referral readiness are tested.
Opening delay points
State licensing review slows launch
Facility inspections can add weeks
Payer credentialing often runs in parallel
Incomplete policies trigger rework
Start before month one
File clinician credentials early
Build EHR workflows before opening
Test intake and claims flow
Recruit for 7 clinicians in year one
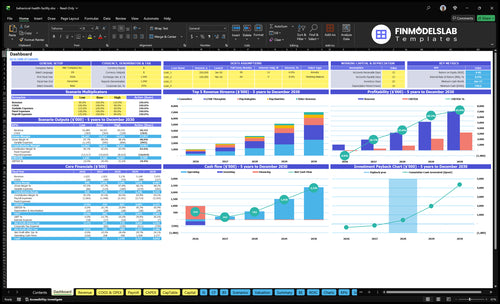
Behavioral Health Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm the behavioral health center opening checklist before accepting patients
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the center is ready to accept patients.
1Compliance
State license activeCritical
You cannot open without the right state license in place.
Local zoning approvedCritical
The site must be allowed to operate as a treatment center.
Clinical director designatedCritical
Clinical leadership needs clear ownership before patient care starts.
Policies and procedures signedHigh
Written rules keep care, escalation, and documentation consistent.
2Facility
Therapy rooms readyHigh
Private rooms need to be set for one-on-one sessions.
Group room compliantHigh
Group sessions need a safe space sized for planned attendance.
Accessibility and safety clearedCritical
Patients and staff need clear access, exits, and safe movement.
Emergency protocol documentedCritical
Crisis steps must be clear before the first high-risk visit.
3Systems
EHR configuredCritical
The EHR system must support charting, notes, and patient records.
Billing and claims liveCritical
Claims need to go out cleanly before revenue starts.
Payment processing testedHigh
Cards and patient payments must work on day one.
Supply budgets within targetsMedium
Year 1 clinical supplies should stay near 15% of revenue.
4Staffing
Core clinician roster filledCritical
Year 1 needs 1 psychiatrist, 1 psychologist, 2 LCSW, 2 counselors, and 1 facilitator.
Credentials and supervision verifiedCritical
Each clinician must be cleared before they see patients.
Coverage schedule lockedHigh
Coverage must match booked visits and crisis response needs.
Admin and billing staff readyHigh
Front desk and billing gaps slow intake, claims, and collections.
5Demand
Referral partners lined upHigh
Referrals matter early because direct demand can start slow.
Local search listing liveMedium
Local search helps patients find the center when they need care.
Payer acceptance confirmedCritical
Accepted plans drive volume and reduce self-pay friction.
Intake script approvedHigh
Clear intake scripts keep screening, scheduling, and routing consistent.
6Cash
Cash runway covers Month 13Critical
Minimum cash is $550k at Month 13, so opening needs a real cushion.
Breakeven month reviewedHigh
Month 14 breakeven means early losses are part of the plan.
Year one loss fundedCritical
Year 1 EBITDA is negative $136k, so launch cash must absorb the gap.
Payback timeline acceptedMedium
The 30-month payback sets the right expectation for investors.
Go-live signoff completeCritical
Do not open until compliance, staffing, systems, and cash are all clear.
Want the six behavioral health center launch drivers?
1Licensing
6-12+ mo
State approval is the go-live gate; no patients until compliance workflows and inspections are cleared.
2Service Model
5 services
A tight outpatient mix sets what you can staff, schedule, and bill without overpromising.
3Clinical Staffing
7 clinicians
Year 1 needs 7 clinicians in place before capacity and supervision coverage can hold.
4Billing Readiness
$85.1K/mo
Billing setup turns care into cash; without enrollment and coding, visits can sit uncollected.
5Referral Pipeline
592/mo
Referral flow drives first-patient volume and helps ramp toward the modeled 592 monthly visits.
6Facility Tech
Pre-open
Rooms, EHR, and intake tools cut opening-month friction and protect privacy and claims.
Licensing And Compliance Approval
Licensing and Approval
This driver decides whether the center can legally open and bill. For a behavioral health center, the gate is state approval, plus zoning, clinical supervision rules, privacy workflows, emergency policies, and inspection status. If any piece is missing, patients should not be accepted. The result is binary: approved and ready, or not open.
The key dependencies are service scope, facility layout, and payer rules. Missing policy evidence is a common bottleneck, and state review can push the launch date back. Until this work is complete, day-one revenue stays at $0, even if staffing and marketing are ready.
Build the approval file first
Start with the approval packet and work backward from inspection. Confirm service category, verify zoning, appoint clinical leadership, complete policies, prepare staff credential files, and test documentation standards before any opening date is set. Keep every item audit-ready so the launch team can answer reviewer questions fast.
Here’s the quick math: if approval slips, the rest of the launch plan cannot convert into revenue. At the modeled $85,140/month revenue run rate, even a short delay matters, so the safer move is to treat compliance as a hard gate, not a side task.
Verify zoning before lease lock.
Name clinical leadership early.
File policies before inspection.
Test charting before first intake.
1
Defined Clinical Service Model
Lock the Service Mix
Day-one care depends on what the center can safely staff and bill. The Year 1 model includes psychiatry, psychology, LCSW therapy, counseling, and group facilitation, with visit pricing from $75 to $250. If the team opens with too many programs, schedules break, intake slows, and staff coverage gets thin.
One service line without a credentialed clinician, room, and payer path is not launch-ready. The real inputs are clinician credentials, room count, payer reimbursement, intake criteria, and referral fit. Medication management can be offered through staff or referral partners, but only if the coverage and handoff process are already mapped.
Build the Billable Menu First
Start with the services you can support on opening day. Map each offering to a named clinician, a room, a schedule block, and a billing path before you publish it. That keeps the opening plan realistic and avoids loading the front desk with requests the clinical team cannot cover.
Use a narrow launch scope and expand later.
Match service to credential.
Cap programs to room count.
Set intake criteria early.
Confirm payer fit before scheduling.
Keep referral partners ready.
If you add group therapy or specialty populations before protocols are set, first-week care gets messy fast. The risk is not just delay; it is weak day-one experience, missed visits, and services that cannot be delivered consistently.
2
Qualified Clinical Staffing
Qualified Clinical Staffing
This launch driver sets whether the center can open with real care capacity on day one. The Year 1 team is 1 psychiatrist, 1 psychologist, 2 LCSW therapists, 2 counselors, and 1 group facilitator, and that mix drives both service depth and payer readiness. If hiring slips or the prescriber is missing, intake, medication-linked care, and visit volume all stall.
Here’s the quick math: modeled utilization supports about 592 visits per month only when the clinical team is fully in place. Readiness is not just headcount; it also means signed offers, license verification, supervision coverage, credentialing files, schedules, intake ownership, and emergency escalation paths. Weak staffing turns opening day into a partial launch.
Verify the clinical team before opening
Build the roster around service mix, payer credentialing, and room capacity, then lock the schedule before you set an open date. The prescriber is the biggest bottleneck: if that seat is late, the center may be staffed on paper but unable to serve the full mix safely or bill cleanly from day one.
Confirm all signed offers first.
File every license and credential.
Map supervision by clinician type.
Assign intake and emergency leads.
Test schedules against room capacity.
What this estimate hides: a full team still needs payer files, documentation standards, and coverage rules aligned. If any one of those lags, the center may open slower than planned, or open with less than 592 monthly visits worth of capacity.
3
Payer And Billing Readiness
Payer And Billing Readiness
Until payer enrollment, Medicaid checks where needed, and private insurance credentialing are done, visits are just care delivered on credit. This launch driver decides whether the center can turn the first day of appointments into collectible cash, not just chart notes. If staff credentials or service codes are missing, claims can’t go out cleanly, and revenue slips into slow accounts receivable.
At target utilization, the model shows about $85,140 per month before fixed overhead. Known variable items add up fast: 25% payment processing, 15% clinical supplies, and 10% therapeutic materials. That’s 50% of revenue before rent, payroll, and other fixed costs, so billing must work from day one.
Bill Before First Visit
Set up the full billing chain before opening: service codes, superbills, claims submission, denial tracking, payment posting, and patient balance rules. The key test is simple: can a real visit be scheduled, coded, submitted, and followed through to payment without manual workarounds? If not, opening day is too early.
Verify payer enrollment status first
Match codes to each service
Check staff credentials against payers
Test denial and payment posting
What this setup hides is timing risk. If claims wait even a few weeks, cash needs rise while visits still happen, and patient balances become harder to collect. The safe launch point is when clean claims can move out on the first day, not after the first month.
4
Referral Pipeline Development
Referral Pipeline
If the center opens without a live referral pipeline, day-one demand stays thin and the first 60-90 days can miss the utilization ramp needed to reach the Year 1 model of 592 visits per month. The pipeline should already include named referral contacts, local search listings, intake phone coverage, an accepted payer list, and enough scheduled assessments to match staffing and clinical eligibility rules.
Referral work covers physicians, hospitals, discharge planners, schools, community providers, employers, employee assistance programs, crisis resources, and local search. Don’t market faster than intake can answer. If outreach starts before service capacity and payer acceptance are set, calls turn into delays, no-shows, and avoidable churn.
Build the intake path first
Before opening, confirm which referrals fit the service model, what payers are accepted, and how fast intake can convert a call into an assessment. Set outreach cadence, assign one owner for each referral source, and test phone coverage during business hours so every lead gets a real response.
Map source, payer, and fit rules.
Keep intake phones staffed.
Track scheduled assessments daily.
Pause outreach if capacity slips.
If assessments are not available quickly, referral volume won’t turn into visits. That slows early revenue and can make the opening look weak even when the clinical team is ready.
5
Facility And Technology Readiness
Care-Ready Facility and Tech
Opening on time depends on whether the site can deliver safe, private, documented care, not just hold chairs and walls. For a behavioral health center, that means therapy rooms, group rooms, accessibility, safety procedures, and a live telehealth setup before the first intake. If any one of those is late, the team may have a licensed site that still can’t see patients.
The tech stack has to be ready at the same time: EHR configuration, intake forms, treatment plan templates, billing integration, phones, payment processing, and vendor contracts. If claims can’t go out cleanly on day one, cash needs rise and the opening month slows. The Year 1 model only works when the center can support about 592 visits per month and collect on about $85,140 per month at target utilization.
Build the room and system stack first
Set up the facility around the clinical model, not the other way around. Match room count to the planned mix of individual, group, and telehealth care, then test documentation flows before opening. One clean mock intake is worth more than a perfect floor plan.
Verify accessibility and safety procedures
Load intake and treatment templates
Test billing and payment posting
Confirm phones and telehealth work
Lock vendor contracts before launch
Watch the dependencies closely: license requirements, the clinical service model, staff schedules, and documentation standards all shape what the site needs on day one. If the site is treated as only real estate, staff friction rises, first assessments slow down, and claims can get messy before the first month closes.
Start with the service model, then work backward into licensing, staffing, facility setup, EHR, billing, and referral readiness The researched plan assumes a 6 to 12+ month launch and a Year 1 team of 7 clinicians At target utilization, that team supports about 592 visits per month, so staffing and referrals must be planned together
Plan for 6 to 12+ months, with state approval, payer credentialing, hiring, and facility readiness driving the schedule The lease may move fast, but the operating approvals usually don’t A center targeting 7 Year 1 clinicians should begin recruiting and credential file preparation well before opening month
Maybe, depending on your state, service type, and payer contracts Some behavioral health or substance abuse programs may need accreditation or payer-specific standards before enrollment or reimbursement Verify this early, because accreditation work can affect policies, documentation, staffing, facility setup, and the launch timeline
Payer credentialing, incomplete billing workflows, weak referral volume, and missing clinical staff delay first revenue In the Year 1 model, revenue depends on 592 monthly visits at modeled utilization and prices from $75 to $250 per treatment If claims or referrals are not ready, those visits will not convert into cash on time
Define the exact clinical services and target population first That choice drives the license, facility layout, clinicians, EHR templates, payer setup, and referral partners A narrow outpatient launch is easier to validate than a broad facility with psychiatry, therapy, counseling, substance abuse services, groups, and telehealth all starting at once
About the author
Eric Dawson
Startup Cost Researcher
Eric Dawson is a startup cost researcher at Financial Models Lab who writes practical guides for founders planning their first business. He focuses on break-even planning and comparing business ideas by cost and effort, with an emphasis on realistic small business planning. Eric’s work keeps attention on useful numbers, clear assumptions, and realistic expectations for business plans.
Choosing a selection results in a full page refresh.