Behavioral Health Center Startup Costs With $177K Monthly Fixed Costs
You’re planning a Behavioral Health Center with therapy, mental health, and substance abuse services, so the opening budget must separate one-time CAPEX from pre-opening costs and working capital This outline uses researched planning assumptions, including $17,700 in monthly fixed costs, $71,667 in monthly Year 1 payroll, and $85,140 in expected monthly revenue during the first operating year
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for opening a behavioral health center, not payroll runway or other non-CAPEX needs.
!
Excluded from CAPEX This calculator covers build-out, furniture, hardware, EHR setup, and security only. It excludes payroll runway, working capital, deposits, debt service, inventory, marketing, payer credentialing delays, reimbursement lag, operating losses, legal costs, and insurance premiums.
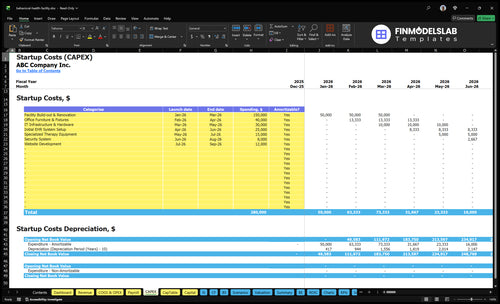
What does the CAPEX and funding screenshot show?
The Behavioral Health Center Financial Model Template screenshot shows CAPEX, startup-cost categories, funding need, launch timing, amounts, and depreciation/amortization. Open model and review assumptions now.
Screenshot highlights
CAPEX and build-out
Staffing ramp and payer mix
Funding need and lag
Behavioral Health Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What drives the cost of opening a Behavioral Health Center?
The biggest cost drivers for a Behavioral Health Center are service intensity, staffing, facility layout, and compliance. A center built for 1 psychiatrist, 1 psychologist, 2 LCSW therapists, 2 counselors, and 1 group facilitator has 7 providers, so it needs more therapy rooms, a group room, private intake flow, sound control, HIPAA privacy, secure records storage, ADA access, safety upgrades, and emergency response planning than a solo office. That facility load sits on top of the $10,000 rent and $700 maintenance line, so the build-out has to match real care delivery, not generic office space.
Build-out costs
7 providers need more rooms.
Group care needs shared space.
Intake needs privacy and flow.
Sound control protects client trust.
Compliance costs
HIPAA drives secure storage.
ADA access rules affect layout.
Substance use services add compliance burden.
Intensive outpatient care adds staffing load.
How do you fund a Behavioral Health Center startup?
Fund the Behavioral Health Center with a split plan: CAPEX, pre-opening costs, working capital, and an operating-gap reserve. With $102 million in Year 1 revenue, 90% variable/direct costs, $860,000 in wages, and $212,400 in fixed overhead, the cash plan has to cover reimbursement lag and staffing ramp. Opening month needs the most runway, then the first operating year, then a five-year growth path as capacity moves from 600% to 700% by provider type and payer mix.
Use of funds
Fund CAPEX first.
Cover pre-opening costs.
Hold working capital cash.
Reserve for operating gap.
Runway logic
Plan for opening month cash burn.
Match staffing to demand ramp.
Model reimbursement lag.
Show five-year growth path.
What hidden costs come with starting a Behavioral Health Center?
Hidden costs in a Behavioral Health Center are mostly working capital, not equipment. For the economics behind it, see How Much Does The Owner Make From A Behavioral Health Center? Opening costs also hit hard in payer credentialing, licensing, accreditation prep, onboarding, EHR setup, billing tests, deposits, and pre-open payroll. The model shows $71,667 monthly payroll, $17,700 monthly fixed costs, and 90% Year 1 variable/direct costs, so even at $85,140 monthly revenue, you’re still looking at about a $142,700 first-year operating gap before one-time CAPEX.
Pre-open cash needs
Licensing takes time.
Credentialing delays cash.
Onboarding costs start early.
Payroll runs before collections.
Cash burn drivers
EHR setup needs testing.
Billing workflow needs fixes.
Marketing starts before revenue.
Referrals take time to build.
Calculate Fuding Needs
Startup cost summary
Startup costs cover build-out, equipment, software, and opening cash needed to launch a behavioral health center.
Highlighted CAPEX$260,000Base planning example
Excluded cash needs$550,000Outside CAPEX total
Funding need$810,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Facility Build-out & Renovation
$150,000
Therapy rooms, group space, ADA access, privacy, and sound control
Yes
Office Furniture & Fixtures
$40,000
Reception, desks, chairs, and waiting area setup
Yes
IT Infrastructure & Hardware
$30,000
Computers, phones, network gear, and secure office systems
Yes
Initial EHR System Setup
$25,000
EHR setup, billing workflow, and launch configuration
Yes
Specialized Therapy Equipment
$15,000
Clinical tools, group room materials, and therapy supplies
Yes
Opening Cash Reserve
$550,000
Year 1 payroll, rent, and fixed-cost runway to breakeven
No
Behavioral Health Center Core Five Startup Costs
Facility Lease, Renovation, And Clinical Build-Out Startup Expense
Lease And Build-Out
Split the startup spend into non-CAPEX items—lease deposit, rent commencement, and architectural planning—and CAPEX leasehold improvements such as walls, sound control, ADA access, safety upgrades, access control, and signage. With monthly anchors of $10,000 rent, $1,500 utilities, $800 insurance, and $700 maintenance, base occupancy is $13,000 per month before payroll.
Floor Plan
Map the floor plan around treatment-room layout, therapy offices, group rooms, assessment space, reception, and check-in flow. For Year 1, ask if the space can support the 1 psychiatrist, 1 psychologist, 2 LCSW therapists, 2 counselors, and 1 group facilitator without bottlenecks. One clean rule: intake should never block therapy starts.
Keep reception close to check-in.
Separate assessment from groups.
Use soundproofing for privacy.
Control Cash
Keep deposits and planning fees off the build-out ledger so you can see true construction CAPEX. Use quotes for architecture, code work, and safety changes, then add contingency for delays and change orders. The usual mistake is overbuilding before staffing and payer flow are stable. That turns cash tied up in space into avoidable stress.
Get contractor pricing before demolition.
Lock scope before signing plans.
Delay extras until ramp-up.
Group Space
Group services and substance abuse programming can need more space than one-on-one therapy. If the room mix is too tight, you get schedule gaps, weak privacy, and slow starts. One-line test: if a group room cannot turn over cleanly, the floor plan is too small for the service mix.
Licensing, Accreditation, Legal, And Compliance Startup Expense
Compliance Setup
Entity setup, licensure, clinical policies and procedures, documentation standards, forms, legal review, payer enrollment support, and compliance consulting sit in this bucket. It also covers HIPAA, the federal privacy rule for protected health information, plus privacy notices, consent forms, and incident reporting. Cost varies by state, service line, payer contracts, and whether you open for outpatient therapy only, IOP/PHP, or substance abuse treatment.
Estimate It
Estimate it by quoting each workstream: filings, license applications, policy manuals, accreditation readiness, and enrollment help. Treat Commission on Accreditation of Rehabilitation Facilities and The Joint Commission as planning categories, not automatic requirements. One-time setup should be separated from ongoing monitoring and renewals, since repeat reviews can add steady admin cost.
Keep It Lean
Use one consultant to draft the base package, then pay counsel only for high-risk review. Reuse templates where state rules allow, but keep payer-specific language and incident steps exact. The biggest cost trap is rework after a state survey, a payer denial, or missing documentation standards.
Plan the Scope
Outpatient therapy only is usually the lightest path; adding IOP/PHP or substance abuse treatment usually means more approvals, tighter policies, and more payer checks. Build the budget around what you will actually launch, not the full menu you may add later, because scope creep drives avoidable legal and compliance spend.
Furniture, Clinical Equipment, And Office Setup Startup Expense
Setup Basics
For a behavioral health center, this spend covers the furniture, computers, phones, printers, secure file storage, and starter clinical supplies needed to open safely. In the model, Clinical Supplies at 15% of Year 1 revenue plus Direct Therapeutic Materials at 10% equals 25%, or about $25.5 million on $102 million of Year 1 revenue.
What It Covers
This line covers therapist office furniture, group room chairs and tables, assessment rooms, waiting room seating, reception, staff workstations, basic screening items if used, routers, office supplies, and first-run therapy materials. Costing starts with unit counts, vendor quotes, and coverage months; the mix changes if you add higher-acuity services.
Count rooms and seats first.
Use vendor quotes, not guesses.
Separate furniture from clinical tools.
Keep It Lean
Buy for an outpatient flow, not a hospital floor. The fastest savings usually come from used desks, simple modular seating, and phased purchases for group rooms, while keeping secure storage, privacy, and basic screening intact. The mistake to avoid is overbuying residential, detox, or hospital-grade gear before the service model needs it.
Outpatient vs. Higher-Cost
Standard outpatient behavioral health usually needs furniture, IT, storage, and low-cost clinical materials. Higher-cost residential, detox, and hospital-grade setups add heavier safety, monitoring, and equipment needs, so their capex can run much higher. One clean rule: only buy what your licensed service mix and room count actually require.
EHR, Billing, Telehealth, Cybersecurity, And Communications Startup Expense
Go-Live Systems
EHR, practice management, billing, telehealth, secure messaging, phones, internet, cybersecurity, permissions, backups, migration, and onboarding must work before launch. Model fixed software cost is $2,000 per month for EHR licensing, $1,200 for operational platform licensing, and $500 for administrative software, or $3,700 monthly. Intake, clinical notes, claims, and compliance depend on it.
Startup Scope
This cost covers setup work, not just subscriptions. Separate monthly licenses from hardware CAPEX and one-time setup or training fees. Get quotes for data migration, workflow buildout, and user training, then map them to launch cash. That keeps the budget honest and shows what you owe before the first client walks in.
Keep It Lean
Match licenses to active users, not wish lists. Set role-based access early, test claim submission and eligibility checks before opening, and turn on backups on day one. The usual mistake is overbuying features or delaying launch until everything feels perfect. That burns cash and pushes intake and billing into manual work.
Cash Drag
Payment processing fees are modeled at 25% of Year 1 revenue, so this layer can hit cash hard even when software spend looks manageable. Fast eligibility checks, clean claim workflows, and tight denial follow-up matter because they cut rework and speed collections.
Staffing Readiness, Recruiting, Credentialing, And Payroll Ramp Startup Expense
Payroll ramp
Pre-opening staffing is a cash sink until claims start paying. Year 1 payroll in the model is $860,000, or about $71,667 per month, before steady collections. That covers psychiatrist leadership, psychology, therapy, counseling, group work, admin, intake, billing support, background checks, credentialing, onboarding, and training.
What it includes
The model assumes 10 clinical director psychiatrist at $250,000, 10 lead psychologist at $150,000, 20 LCSW therapists at $90,000 each, 20 counselors at $75,000 each, 10 group facilitator at $80,000, and 10 administrative assistant at $50,000. Use these counts and rates to size launch payroll and to separate pre-opening hiring from ongoing operating payroll.
How to stage it
Hire in step with capacity ramp and payer credentialing, not just the org chart. If credentialing slows, collections lag but payroll does not, so the burn rate stays high. Keep intake and billing coverage lean at launch, then add staff as reimbursement clears and caseloads fill.
Credential before scaling full panels
Train before open, not after
Match hires to live demand
Cash timing risk
What this estimate hides: payroll starts before steady collections, so even a good team can strain cash if payer enrollment or credentialing slips. The safe move is to treat launch labor as a startup cost, then move only the roles tied to live referrals and approved billing into the operating run rate.
Compare 3 Startup Cost Scenarios
Scenario table
A small outpatient clinic, the researched base model, and a larger IOP/PHP build need very different capital. Use the ranges to match rooms, staffing, and reserve depth to the launch plan.
Lean, Base, and Full launch scenarios for a behavioral health center.
Scenario
Lean LaunchSmall clinic, low complexity
Base LaunchBalanced clinic, moderate complexity
Full LaunchProgram scale, high complexity
Launch model
Open a small outpatient clinic with fewer rooms, lighter group programming, and a lean pre-opening team.
Open the modeled outpatient center with 1 psychiatrist, 1 psychologist, 2 LCSW therapists, 2 counselors, and 1 group facilitator.
Open a larger IOP/PHP-style program or substance use track with more group rooms, tighter compliance, and a larger reserve.
Typical setup
Use only the core therapy rooms, limited group space, and the minimum clinical and admin staff needed to start.
Use the model's staffing mix, planned room count, and standard EHR, billing, and admin tools.
Use more treatment space, heavier documentation, and more front-office, billing, and clinical coverage.
Cost drivers
Build-out
furniture
core staff
EHR setup
opening cash
Build-out
payroll
rent and utilities
software stack
referrals
More rooms
higher payroll
compliance work
systems setup
reserve depth
Planning rangeCAPEX only
$250,000 - $450,000Light capex, light reserve
$500,000 - $750,000Mid capex, mid reserve
$900,000 - $1,400,000Heavy capex, heavy reserve
Best fit
Best for founders starting with a smaller outpatient panel and modest group volume.
Best for teams using the researched operating model as their launch target.
Best for operators building a broader program with more intensity and volume from day one.
!
Planning note: These ranges are researched planning assumptions from the model, not exact quotes or national averages.
The researched model does not include one-time vendor CAPEX quotes, so don’t treat it as a full all-in price It does show the operating funding base: $17,700 in monthly fixed costs, about $71,667 in monthly Year 1 payroll, and $85,140 in monthly revenue at early capacity Add facility build-out, licensing, legal, technology setup, and working capital on top
It can affect the early ramp-up period because visits may start before steady collections arrive The model already shows tight cash flow: $85,140 in monthly Year 1 revenue against about $89,367 in payroll and fixed overhead before variable costs If reimbursement is slow, the working capital reserve needs to cover payroll, rent, EHR, insurance, and billing delays
It depends on the state, service line, payer contracts, and whether the center offers outpatient therapy, IOP/PHP, or substance abuse treatment Accreditation preparation can affect legal, compliance, policies, training, and documentation costs Budget it separately from CAPEX because it does not buy furniture or build rooms, but it can still delay opening and cash collections
Lease planning should start with treatment flow, not just price per square foot The model assumes $10,000 per month in rent, plus $1,500 utilities, $800 facility insurance, and $700 maintenance The space must support private therapy, group sessions, intake, ADA access, privacy, sound control, and secure records, or cheap rent can become expensive build-out
Reserve enough to cover the early gap between payroll, rent, billing setup, and collected revenue In the researched model, Year 1 revenue is about $102 million, but wages are $860,000, fixed overhead is $212,400, and variable/direct costs equal 90% of revenue That creates an estimated $142,700 first-year operating gap before one-time CAPEX and reimbursement timing risk
About the author
Ryan Spencer
First-Time Founder Guide Writer
Ryan Spencer writes for Financial Models Lab, where he focuses on launch budget planning and simple launch planning for first-time founders. He helps readers estimate startup needs before opening a physical location, breaking down business costs in clear, practical language. His work is built for people who want a realistic view of what it really takes to open a business, so they can plan with more confidence and fewer surprises.
Choosing a selection results in a full page refresh.