 Time to Open6-12 weeksSetup window
Time to Open6-12 weeksSetup windowHow To Start A Healthcare Denial Management Service In 6–12 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 weeksSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckAccess gatePayer portals
Key BottleneckAccess gatePayer portals First Revenue StepSigned clientQueue begins
First Revenue StepSigned clientQueue begins


To start a denial management business, pick a provider niche, prepare HIPAA controls, sign business associate agreements, build appeal workflows, secure payer and billing system access, hire trained denial staff, and launch with one or two pilot providers A realistic researched planning assumption is 6–12 weeks to open if compliance, staffing, and client data access are ready The main bottleneck is not the website it’s getting secure access to denial queues, payer portals, remittance files, and medical records In the model, first revenue comes from subscription contracts ranging from $1,500 to $7,500 per month, with breakeven projected in Month 9
Time to Open6-12 weeksSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckAccess gatePayer portalsFirst Revenue StepSigned clientQueue beginsLaunch timeline
Short web summary of the launch plan; the XLSX export carries the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Legal and compliance
- Form entity
- HIPAA policies
- Sign contracts
- Bind insurance
Operations workflow
- Denial categories
- Appeal templates
- Reporting format
- QA checklist
Technology and payer access
- Secure systems
- Billing access
- Payer portals
- Remittance feeds
Staffing and training
- Hire analysts
- Assign account manager
- Train coding review
- Shadow cases
Provider sales
- Target accounts
- Build lead list
- Outreach sequence
- Close pilot
Pilot launch
- Intake aged denials
- Queue current denials
- Launch pilot
- Review outcomes
Why test the launch plan before signing providers?
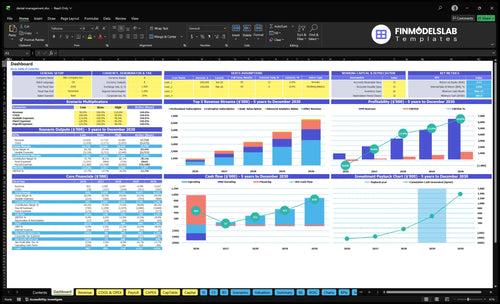
Dashboard and assumptions tabs show revenue, costs, cash needs, and break-even logic; EBITDA goes from -$257k in Year 1 to $138k in Year 2. Open the Healthcare Denial Management Service Financial Model Template.
Financial model highlights
- 40/50/10 Year 1 mix
- 15% add-on attach
- 8% cloud, security
- 10% commissions, referrals
- $386k cash floor
- Month 43 payback
How long does it take to start a denial management service?
A Healthcare Denial Management Service usually takes 6–12 weeks to launch, not a fixed promise. It can move faster when HIPAA policies, contracts, secure systems, and experienced denial analysts are already in place; it slows down when EHR or billing access, payer portal credentials, test reporting, coding review, or pilot approval lag. Here’s the quick math: the model assumes operations begin in Month 1, breakeven lands in Month 9, and Year 1 revenue reaches $953k.
Faster launch path
- Start with aged denial queues.
- Finish HIPAA before PHI intake.
- Set workflows before appeal volume.
- Use existing secure systems and analysts.
Delay drivers
- Waits for EHR and billing access.
- Needs payer portal credentials first.
- Test reporting can hold go-live.
- Expand only after recurring reporting works.
What denial management launch mistakes put provider trust at risk?
The biggest trust risk is weak setup: bad HIPAA controls, no BAA process, vague scope, and unclear SLAs. If onboarding takes 14+ days after contract because access is blocked, churn risk rises, so the Healthcare Denial Management Service should prove readiness before promising recovery outcomes.
Trust checks first
- Test PHI access
- Confirm payer portal permissions
- Review appeal templates
- Define escalation path
Launch controls
- Set reporting cadence
- Assign quality control
- Use dashboard metrics
- Track denial prioritization
What do you need to start a denial management service?
To start a Healthcare Denial Management Service, you need the operating stack before the sales stack: HIPAA controls, a business associate agreement with each provider client, secure claim-file handling, payer portal access, and a documented appeal workflow; How Launch Healthcare Denial Management Service? should start with those basics. The baseline model needs 6 Year 1 roles, reaches breakeven in Month 9, and shows minimum cash of $386k in Month 17.
Launch stack
- Sign BAAs: business associate agreements
- Secure claims, EOBs, remittance data
- Track medical records and appeals
- Define client contract and reports
Operating needs
- Hire CEO and 3 specialists
- Add account manager and sales executive
- Build coding review path
- Blocker: no secure payer access
Denial management launch readiness checklist objective
Launch readiness checklist
Use this go-live approval checklist before opening to confirm compliance, systems, staffing, and first-client readiness.
Compliance
- Entity setup completeCritical
You need a legal entity before contracts, insurance, and payments.
- HIPAA policies approvedCritical
PHI handling must be written before any client data moves.
- BAA workflow readyHigh
Every provider and vendor touching PHI needs a signed path.
Security
- Secure systems hardenedCritical
PHI access needs encryption, backups, and locked-down devices.
- User access rules setCritical
Only approved staff should see claim and patient data.
- Payer portal process testedHigh
Appeals stall if portal steps and credentials are not ready.
Workflow
- Denial categories mappedHigh
Clear buckets make appeal work faster and more consistent.
- Appeal templates approvedHigh
Standard letters keep the team from rewriting each case.
- Escalation path definedMedium
Complex denials need a fast path to senior review.
Team
- Year 1 roster approvedCritical
The launch plan needs CEO, 3 specialists, manager, developer, and sales exec.
- Specialists trained on appealsHigh
Staff must know coding review, docs, and payer rules.
- Account handoff trainedMedium
Clean handoffs keep clients updated and reduce missed follow-ups.
Sales
- Provider pilot list approvedHigh
First revenue depends on a short list of provider pilots.
- Client contract readyCritical
Terms must cover scope, PHI handling, and service limits.
- Pipeline reporting liveMedium
The team needs weekly counts on leads, pilots, and closes.
Finance
- Cash runway modeledCritical
The plan needs $386k minimum cash through Month 17.
- KPI dashboard liveHigh
Track denial rate, overturn rate, dollars recovered, and aging.
- Go-live signoff completeCritical
Start only after compliance, systems, staffing, and sales are all ready.
Want to see the six launch drivers that decide go-live?
1HIPAA Readiness
BAA gateSigned BAA, security controls, and audit cadence shorten legal review and let protected data move sooner.
2Claims Access
Portal accessSecure access to portals and claims files starts appeals faster and avoids a signed-contract stall.
3Appeal Playbooks
Appeal flowClear denial rules and appeal templates keep the team on high-value claims from day one.
4Qualified Staff
7 FTETrained staff and quality review reduce weak appeals and make early service delivery reliable.
5Results Reporting
Results dashboardA live results dashboard shows recoveries and overturns, which makes renewals and expansions easier.
6Pilot Strategy
Pilot winsA tight niche offer and pilot contract bring in first revenue faster and keep onboarding simple.
HIPAA And Contract Readiness
HIPAA And Contract Readiness
If you want to handle protected health information, the business is not launch-ready until the client contract is signed and the business associate agreement (BAA) path is in place. Without that, you can’t safely start denial work, and a provider will likely slow or stop onboarding before the first claim review.
This driver covers data security policies, access controls, insurance, audit cadence, vendor review, breach response, user permissions, and secure file exchange. The risk is simple: weak controls lose trust early, and that can delay go-live even when sales are already closed. No BAA, no PHI.
Contract-First Setup
Start with legal review and provider approval, then lock the operational pieces that prove you can handle PHI safely. Make sure the contract, BAA workflow, policy set, and vendor list are ready before any live data moves. That keeps onboarding fast and cuts back-and-forth during contracting.
Before launch, verify user permissions, secure file exchange, breach response steps, and the audit cadence. Then test the handoff with a sample file, so the team knows who can see what, where files go, and how issues are escalated. Clean controls now reduce delays later.
- Sign contract before PHI access.
- Approve BAA process early.
- Document security and breach steps.
- Limit access by role.
- Test secure file exchange.
1
Payer And Claims Data Access
Payer and Claims Access
This driver decides whether the service can actually start. Even with a signed contract, you are not live until you have secure access to denial queues, remittance data, explanations of benefits (EOBs), medical records, payer portals, clearinghouse files, and the client’s billing system. Without those feeds, the team can’t review denials, build appeals, or produce a first report.
The main launch risk is admin delay. Provider administrators or payer credentials can stall access, so the calendar says open while operations are still blocked. The quick test is simple: if you can pull a live denial file and start appeal work, you’re ready; if not, the go-live date slips and first cash recovery starts late.
Lock Access Before Go-Live
Treat access like a launch workstream, not a side task. Build an access request workflow, set role-based permissions, name one escalation owner, and keep an intake checklist for test files and production files. That keeps onboarding from getting stuck between contract approval and IT setup.
- Confirm denial queue access first.
- Then verify payer portal credentials.
- Request remittance and EOB files.
- Test medical record and billing access.
- Document who approves each request.
When access is clean, appeals start faster and the first reports are cleaner because the team is working from the same source files from day one.
2
Denial Workflow And Appeal Playbooks
Denial Workflow Playbooks
Your opening date depends on whether the team can sort denials fast and the same way every time. A clear denial workflow is the operating backbone: category rules, priority rules, documentation standards, appeal letter templates, escalation paths, and payer-specific follow-up rules. Without that, day-one work gets messy, and the first claims can sit in the wrong queue.
This launch driver also sets the service tone with providers. If the team starts with medical necessity, coding, prior authorization, timely filing, and eligibility denials in the wrong order, lower-value claims can crowd out recoverable ones. The business needs access to EOBs, medical records, claim history, and coding review before go-live, or the first reports will be slow and weak.
Set the claim triage rules first
Before opening, lock the workflow in writing and test it on sample denials. Define how each denial type is tagged, who owns it, what evidence is required, and when it escalates. That means one playbook for medical necessity, one for coding, one for prior authorization, and clear follow-up timing for each payer.
Also assign a rule for what gets worked first so staff do not burn time on low-value claims. The launch is ready when a new denial can move from intake to letter draft to payer follow-up without debate. That is what creates cleaner handoffs and better provider visibility from day one.
- Tag denials by type before review.
- Require EOB and claim history access.
- Use one appeal template per denial type.
- Set payer follow-up deadlines in writing.
- Escalate weak or high-value claims fast.
3
Qualified Denial Management Staffing
Qualified Denial Staffing
Staffing is the go-live gate here. This service lives or dies on trained denial analysts, coding support, account ownership, and quality review before the first pilot claim hits the queue. If people are undertrained, appeals get weak, payer follow-up slows, and the provider sees sloppy recovery work instead of reliable service.
The Year 1 salary plan is $645,000 total: 3 denial management specialists at $65,000 each, 1 account manager at $75,000, 1 software developer at $115,000, 1 sales executive at $85,000, and CEO at $175,000. A founder-led start can trim early headcount, but that usually shifts the risk to delivery capacity and slower provider trust.
Staff Before First Volume
Lock the operating roles before launch. Decide who reviews denial coding, who writes appeals, who owns client communication, and who signs off on quality. That setup matters more than raw headcount, because day-one mistakes in denial logic or payer follow-up can stall recovery and hurt first impressions.
- Assign a named owner for each appeal.
- Train staff before pilot claims arrive.
- Build QA checks into every file.
- Keep the founder out of bottlenecks.
- Test workload against launch volume.
If one person is doing analysis, coding, and client updates, the team can open on time but still miss service levels. The cleanest signal is simple: trained staff, clear handoffs, and quality review in place before the first provider goes live.
4
Reporting And KPI Infrastructure
Denial KPI Dashboard
If you open without a clear reporting stack, the team may recover money but fail to prove it. For this service, the launch risk is not just doing the work; it’s showing denial rate, appeal overturn rate, dollars recovered, and aging from day one so clients see value fast and stay past the pilot.
The readiness signal is a dashboard or report built from claims data, remittance files, appeal status, and provider feedback. The first deliverables should be a baseline report, weekly pilot updates, and a monthly executive summary, plus root-cause tracking for preventable denials and prevention recommendations.
Lock the Data Feeds First
Before launch, verify that each client can send clean files and that your team can validate them. If the claim file, denial codes, or appeal status lag by even a few days, the dashboard goes stale and the client’s trust drops. That delay also pushes back renewal proof and the case for the $500 monthly analytics add-on in Year 1.
Build the report around a simple sequence: ingest, validate, tag root cause, then publish. Keep one owner on data checks and one on client updates, so the first report does not depend on a scramble. A clean first cycle matters more than fancy charts.
- Track preventable denials weekly.
- Show recovery dollars in plain dollars.
- Flag old appeals before they age out.
- Link each KPI to a fix.
5
Provider Acquisition And Pilot Contract Strategy
Pilot Offer And Target Fit
This launch driver matters because a denial management service opens on time only if the first offer is narrow enough to sell and deliver. If the pitch drifts into broad revenue cycle management, you slow sales, blur scope, and delay the first claim review. Use a niche target, a denial audit script, and a pilot contract so the first client can say yes fast.
The Year 1 anchors are $1,500, $3,500, and $7,500 per month, with a $120k marketing budget and stated $2,400 CAC. That implies about 50 clients if CAC holds ($120,000 / $2,400). If the scope, service levels, and first report format are not locked before outreach, onboarding slips and first revenue gets pushed back.
Lock Scope Before Selling
Before opening, verify the pilot contract covers the denial types, the data needed, response timing, the first report format, and the success metric. That keeps sales honest and gives ops a clean day-one handoff. One clear scope note can save a week of back-and-forth.
- Denial categories and exclusions
- Service-level agreement timing
- Pricing: retainer, per-claim, or performance
- Required claims and payer data
- First report layout and due date
Start every sales call with a denial audit script. If the client cannot confirm denial volume, claims access, and a payer follow-up owner, pause the pilot. That is the real launch gate. It protects cash, keeps the work focused, and stops the first month from turning into unpaid custom work.
6
Related Products
- Healthcare Denial Management Service Porter's Five Forces Analysis
- Healthcare Denial Management Service BCG Matrix
- Healthcare Denial Management Service Business Model Canvas
- What Are The 5 KPIs For Healthcare Denial Management Service Business?
- Healthcare Denial Management Service Business Plan Template in Pre-Written Word
- How Increase Profits For Healthcare Denial Management Service?
- What Are Operating Costs For Healthcare Denial Management Service?
- Healthcare Denial Management Service Startup Costs: $235K CAPEX
- Healthcare Denial Management Service Financial Model Template in Excel
- How Much Healthcare Denial Management Owners Make At $953k Revenue
- How To Write A Business Plan For Healthcare Denial Management Service?
- Healthcare Denial Management Service Marketing Mix
- Healthcare Denial Management Service Marketing Plan
- Healthcare Denial Management Service Business Proposal
- Healthcare Denial Management Service PESTEL Analysis
- Healthcare Denial Management Pitch Deck Example Editable PPTX
- Healthcare Denial Management Service Business SWOT Analysis
- Healthcare Denial Management Service Value Proposition Canvas
Frequently Asked Questions
Start with a provider niche, HIPAA controls, business associate agreements, secure claims intake, payer access, trained denial analysts, and a pilot contract The researched launch window is 6–12 weeks when staffing and access are ready The model assumes Year 1 revenue of $953,000 and breakeven in Month 9, so validate operations before scaling sales