How To Open A Dental Clinic: 6 To 12 Month Launch Plan
You’re launching a healthcare site before the first patient can sit in the chair, so sequencing matters This dental clinic launch plan covers the 6 to 12 month path through licensing, lease, build-out, equipment, staffing, credentialing, compliance, and first appointments, with model checks for the first operating year
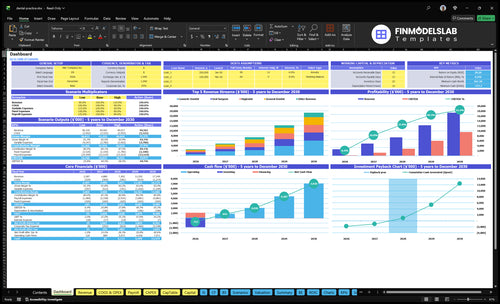
Time to Open10 monthsSetup windowLaunch Sequence8 stagesLicense firstKey BottleneckBuildout delayLead timeFirst Revenue StepNew examsBooking live
Dental clinic launch timeline
This web summary shows the launch path in 12 months, and the XLSX export includes the detailed Gantt Chart.
How do you get first patients for a dental practice?
Get the first patients by chasing booked appointments, not vanity marketing, and start with Google Business Profile, local search pages, insurance directories, referrals, community outreach, launch offers, online booking, and a strong phone script. For a quick cost view, see How Much Does It Cost To Open And Launch Your Dental Clinic? The first revenue should come from new-patient exams, hygiene visits, restorative consults, and treatment-plan follow-up, while a soft opening keeps flow tight so staff can test intake, imaging, sterilization, payment collection, and claims submission.
Start with access
Claim Google Business Profile first
Build local search pages
List in insurance directories
Use online booking and phone scripts
Fill the calendar
Push new-patient exams first
Book hygiene and restorative consults
Use referral and outreach offers
Track conversion from day one
How long does it take to open a dental clinic?
Opening a Dental Clinic usually takes 6 to 12 months, and the real date is the latest unresolved dependency, not the first task. Site selection, lease terms, design, permits, build-out, plumbing, electrical, radiation shielding, chair install, imaging setup, inspections, hiring, credentialing, and claims testing all sit on the critical path. A smaller one-provider launch can move faster, but staffing should be ready before the soft opening, not after.
What slows opening
Site and lease terms set the pace.
Permits and inspections add delay.
Build-out can hold the critical path.
Credentialing can delay first revenue.
What must be ready
Plumbing and electrical work must pass.
Dental chairs and imaging need install and test.
Staffing should be in place before opening.
Claims testing should happen before patients arrive.
What do you need to open a dental clinic?
To open a Dental Clinic, secure legal permission first: active provider licenses, a business entity, lease, permits, x-ray registration, malpractice coverage, OSHA systems, HIPAA systems, and infection-control controls; then prepare equipment, software, staffing, billing, and intake before seeing patients. Track readiness against patient access and revenue metrics like What Is The Most Important Measure Of Success For Your Dental Clinic?; this model starts Year 1 with 7 clinical providers and 7 support roles serving patients within a 10-mile radius.
Must-Haves First
Confirm state dental board rules
Register business entity and lease
Secure permits and x-ray registration
Set OSHA, HIPAA, sterilization systems
Launch Setup
Staff 2 general dentists
Add 2 hygienists and specialists
Hire 7 support staff
Set scheduling, billing, intake, payments
Key Takeaways
Licensing and x-ray clearance decide legal opening.
Build-out delays can push equipment and launch dates.
Billing setup turns booked visits into cash.
Soft opening protects workflow before full demand.
Licensing and compliance
Licensing clearance
A dental clinic cannot open on time if it lacks active dental licenses, state board approval, and local permits. This is the gate that lets you diagnose, treat, image, document, and bill. If x-ray registration or infection control paperwork is missing, you can have chairs installed and still be unable to run full new-patient exams.
The real dependencies are provider credentials, facility setup, equipment choices, and payer enrollment. That makes compliance a launch-path item, not a back-office task. If you miss it, the clinic may open in a limited mode, with slower cash flow and more claim or regulatory risk.
Lock compliance before scheduling
Assign one owner for licensing, then verify the state dental board checklist, business registration, malpractice insurance, OSHA training, HIPAA policies, sterilization logs, radiography rules, and local approvals. Build the exposure control plan, document patient privacy rules, and validate sterilization before the first patient is booked.
Confirm active provider licenses.
Test x-ray clearance early.
Document infection control workflows.
Match payer enrollment to licenses.
Keep the launch plan tied to what can be legally done on day one. A clinic with chairs installed but no radiography clearance cannot finish full exams, which slows intake and pushes the opening toward a partial launch instead of a clean start.
1
Location and build-out
Clinic Build-Out
For a dental clinic, location and build-out decide whether the office can actually serve patients on day one. A signed lease is only the start; the space still needs a usable floor plan, permits, contractor timing, and room for imaging, sterilization, staff work, and patient flow. If plumbing, electrical, compressor, vacuum, or shielding is wrong, opening slips and equipment install gets blocked.
The site also has to support parking, visibility, and inspections. A good traffic corner with weak utility capacity can still become a bad launch if it forces redesigns or change orders. That is how a simple site choice turns into a longer 6 to 12 month path to opening.
Lock the site before ordering gear
Start with the physical constraints, not the décor. The clinic layout has to fit operatories, sterilization flow, and imaging before you commit to equipment dates or opening day. One clean rule: no final equipment plan until utilities and permits are matched to the floor plan.
Confirm landlord approval in writing.
Match plumbing to chair count.
Verify electrical and compressor capacity.
Plan shielding if radiography needs it.
Sequence permits before contractor start dates.
Keep inspections tied to build milestones.
Assign one owner to track the contractor schedule, permit status, and utility sign-offs. If the office cannot pass inspection on time, hold back equipment delivery and soft-opening bookings. One missed utility check can push opening day and slow first revenue before the team is ready.
2
Dental equipment and clinical systems
Dental Equipment and Systems
This driver decides whether the clinic can treat patients on day one. Installed operatories, chairs, compressors, vacuum systems, imaging, sterilization equipment, supplies, phones, payment systems, and the EHR/practice management setup all have to work together. If one link fails, multiple chairs can sit idle; one ready chair with imaging offline slows exams and treatment plans.
Launch readiness is more than delivery. You need validated installation, tested workflows, and confirmed sterilization cycles before the first visit. That matters because Year 1 provider capacity starts at 45% to 60%, so any equipment delay cuts usable capacity fast and pushes first revenue out.
Test Before First Patient
Sequence this after build-out completion and the checks for power, plumbing, software setup, and staff availability. Assign one owner to track delivery, install, training, stock levels, and mock visits so no chair opens half-ready.
Verify each operatory works end to end.
Test imaging before new-patient exams.
Run sterilization cycles and log results.
Practice phones, payments, and check-in.
What this hides: one failure can block several chairs, so the clinic should not open until the bottleneck system is fixed and staff can move through a full visit without stopping.
3
Staffing and training
Staffing and training
This matters because a dental clinic can’t open smoothly without provider coverage, trained dental assistants, and front-desk help in place. If hiring slips, visits run long, handoffs break, and collections get messy on day one.
The weak spot is usually the front desk. A full clinical schedule with only one trained front-desk person can hurt check-in, claim accuracy, and treatment-plan follow-through, which slows cash and frustrates patients. Late hires also delay the soft-opening schedule and raise the risk of missed calls, missed notes, and missed revenue.
Staff the launch lane
Before opening, confirm software access, compliance training, and payer setup for every role that touches patients or billing. Then test the full flow: phone script, intake process, treatment-plan handoff, and emergency roles. That keeps the team ready for first visits, not just hired on paper.
Assign a clinic director.
Train assistants on room flow.
Cover front desk and billing.
Confirm specialist coverage if used.
Run one mock day before opening.
Use the Month 1 plan to lock in patient care coordinators, dental assistants, general dentists, hygienists, a cosmetic dentist, and a marketing coordinator. The goal is simple: every chair, call, and claim has an owner before the first patient walks in.
4
Payer credentialing and billing setup
Payer Credentialing and Billing
This driver decides whether booked visits turn into collectible revenue on day one. It covers payer enrollment status, fee schedules, claims workflows, coding setup, payment processing, patient financing, eligibility checks, and treatment-plan presentation. No active payer setup, no clean first claim.
For a dental clinic, the risk is simple: if you open before credentialing clears, you may be forced into cash-pay only, delay claims, or confuse patients about what they owe. With provider capacity starting at 45% to 60% in year one, every early visit needs a working billing path to protect cash flow.
Pre-Open Billing Checks
Before launch, verify the basics in order: provider licenses, entity setup, tax details, software access, and bank accounts. Then submit credentialing packets, load fee schedules, test claim submission, train staff on estimates, set payment policies, and reconcile deposits. If any one step slips, first revenue slows even when the schedule is full.
Confirm payer enrollment status first.
Test one clean claim end-to-end.
Train front desk on estimates.
Set payment rules before opening.
Check eligibility before every new visit.
Watch directory listings for live status.
A common failure case is hygiene already booked but insurance directory listings are not live yet. That slows first-patient volume and creates confusion at check-in. The goal is simple: make the first appointment collectible, not just scheduled.
5
Patient acquisition and soft opening
Patient acquisition and soft opening
This driver decides whether the clinic opens to a full chair map or to empty slots. Live Google Business Profile, local search, insurance directories, and referral outreach need to be ready before the first day so the front desk can book new-patient exams, hygiene visits, and restorative consults. If marketing turns on before phones, software, or payer status are ready, demand outpaces service and the launch slips.
The key dependency is opening date confidence. Soft opening capacity should stay controlled until provider schedules, phone coverage, review flow, and billing are tested. That matters because the Year 1 model assumes usable capacity starts at only 45% to 60%, so filling every chair on day one can expose sterilization, check-in, and claim errors instead of building steady first revenue.
Launch in small waves
Build launch pages, confirm directory listings, and train the front desk before any promotion goes live. Then call nearby referral sources, set a review process, and book a limited mix of new-patient exams, hygiene visits, and restorative consults so the team can test phone coverage, intake, and handoffs without overfilling the schedule.
Use the soft opening to verify what breaks under load: booking speed, insurance checks, charting, and chair turnover. If the software or billing workflow slows the day, cap appointments and fix the bottleneck first. That keeps first-patient flow aligned with the revenue ramp instead of creating a full waiting room and a stressed back office.