How To Open A Disability Care Service In 60 To 120+ Days
You’re opening a disability care service before taking clients, so the work is compliance, staffing, referrals, and day-one operations This launch plan covers a 60 to 120+ day opening path, a 5-year planning period, and a service mix led by in-home assistance, life skills development, and community engagement Next, confirm state rules and payer requirements before you hire into fixed costs
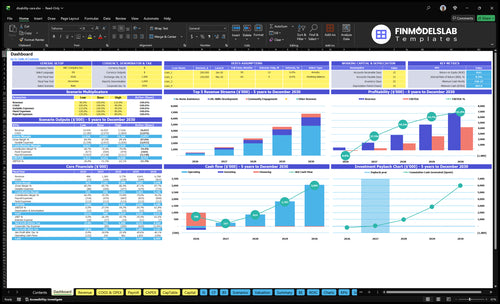
Time to Open8-16 weeksSetup windowLaunch Sequence6 stagesScope firstKey BottleneckLicense gateApproval pathFirst Revenue StepBooked visitCare plan ready
Launch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
What mistakes cause disability care launch problems?
Disability Care Service launch risk spikes when sales outruns staffing. Don’t sell hours you can’t safely staff; lock in caregiver schedules, backup coverage, individualized service plans, emergency steps, and reporting before the first visit. That usually means fewer cancellations, cleaner claims, and stronger referral trust.
Fix coverage first
Confirm caregiver schedules early
Set backup coverage now
Match each client plan
Define service boundaries clearly
Fix compliance next
Prepare incident reporting
Train abuse and neglect reporting
Keep client records current
Test billing and referral follow-up
How long does it take to open a disability care service?
Opening a Disability Care Service usually takes 60 to 120+ days, and that is a practical enrollment timeline, not a guaranteed opening date. The clock stretches when state review, Medicaid waiver approval, background checks, insurance binding, policies, and billing workflows are still unfinished. Client onboarding should wait until care plans, scheduling, documentation, payroll, and incident reporting are live.
Main delays
60 to 120+ days is the real window.
State review can slow launch.
Background checks must clear first.
Policies and billing need testing.
Launch readiness
Private-pay may open faster.
Payer-funded services need enrollment ready.
Care plans should be live before onboarding.
Scheduling and incident reporting must work.
Do you need a license to start a disability care service?
Yes—your Disability Care Service will often need approval before serving or billing clients, but the exact license depends on your state, care type, service scope, and payer source. Treat licensing as a launch gate, not paperwork; see What Is The Current Growth Trend Of Your Disability Care Service? because missing approval can block Medicaid waiver billing, private-pay referrals, and service start dates.
Check Licensing First
Verify state disability care agency rules
Separate non-medical care from skilled care
Confirm respite and habilitation requirements
Plan for inspections before launch
Clear Billing Gates
Complete Medicaid waiver provider enrollment
Run required background checks
Set training and incident reporting standards
Serve a market of 44.1 million disabled Americans
Key Takeaways
Licensing approval comes before referrals, billing, and opening.
Service scope should match state rules and payer limits.
Policies, training, and documentation cut care and billing risk.
Staffing and intake workflows must be ready on day one.
Licensing And Payer Approval
License and Payer Gate
For disability care, no written approval means no real launch. State licensing and Medicaid waiver provider enrollment decide whether you can open on time, bill correctly, and take the first client without claim denials or referral delays.
Check the exact service scope first, because non-medical support, personal care, and skilled care can trigger different rules. The readiness signal is simple: written approval or clear authorization for the service you will sell and the payer path you will use.
Clear the Approval Path Early
Before opening, line up entity setup, license application, payer enrollment, insurance certificates, compliance files, and renewal tracking. Also verify background checks, training rules, documentation standards, and any inspection or enrollment steps tied to your state.
Use a tight launch file so nothing stalls at the end. A clean setup can also cover fixed admin costs like $1,000 monthly for client software, $1,800 monthly for liability and workers comp insurance, and $600 monthly for regulatory compliance and licensing.
Confirm state rules by service type.
Match payer rules before marketing.
Track renewals before they expire.
Keep records ready for inspection.
Delay intake until approval is clear.
1
Service Scope
Define the Service Menu
Scope decides who you can take, what caregivers can do, and whether you can open on time. If the menu is loose, intake may promise work that needs extra licensing or payer approval, which delays launch and creates compliance gaps. Year 1 should be built around 70% in-home assistance, 40% life skills development, and 25% community engagement.
The launch gate is a written menu with eligibility, visit types, caregiver duties, exclusions, and escalation rules. Map personal care, respite, community support, and life skills work to state and payer requirements before marketing starts. That gives cleaner referrals, better staffing, and fewer surprises on day one.
Lock the menu before intake
Build a service matrix before you hire or sell. For each service, write what the agency does, who qualifies, what caregivers may do, and what needs a licensed clinician. Then remove anything that would trigger a separate license, extra training, or payer approval. That keeps the launch plan tied to real capacity, not wishful thinking.
Test the scope against the first five client types you expect to serve. If a task falls outside the written menu, route it to escalation or exclude it. A tight scope makes onboarding faster, training simpler, and first visits safer because staff know the boundary before the schedule starts.
Write exclusions first.
Match tasks to state rules.
Separate licensed from nonlicensed work.
Use one intake script.
Train staff on escalation rules.
2
Policies, Documentation, And Risk Control
Policies and Records
Policies and records are day-one operating infrastructure, not an inspection binder. For a disability care agency, launch is gated by complete intake forms, individualized service plans, medication boundaries, emergency protocols, abuse-and-neglect reporting, incident logs, caregiver notes, and quality checks ready before the first visit. If those items are missing, staff improvise, and care risk starts on day one.
The dependency is simple: your documents must match state rules, payer standards, insurance requirements, and service scope. That means defining what gets written, who reviews it, how issues escalate, and where client records are stored. Weak documentation can trigger care errors, complaints, or delayed billing, so the business may open on paper but not operate cleanly.
Set the file system before first client
Start with one file standard and one review rhythm. Every client record should capture intake, the service plan, visit notes, incidents, and escalation steps. Then test the full flow: caregiver writes it, supervisor reviews it, and billing can use it without chasing missing data. If that chain breaks, fix it before taking referrals.
Define note templates now.
Assign a daily review owner.
Set escalation rules in writing.
Store records in one system.
Train staff on reporting rules.
The real launch risk is not paperwork volume; it is missing or inconsistent records that slow billing and weaken compliance protection. A clean policy set helps the team deliver safer care, document it the same way every time, and avoid first-month surprises when claims or complaints hit.
3
Caregiver Staffing And Scheduling
Caregiver Coverage First
Don’t hire caregivers until the first confirmed service commitments are in hand and the schedule can actually be covered. For this model, each active customer averages 15 billable hours per month, so the launch risk is simple: if coverage is thin, you miss visits, delay start dates, and damage trust on day one.
Background checks, screening, role-specific training, and backup coverage are launch gates, not nice-to-haves. With direct caregiver wages modeled at 12% of revenue and specialized training at 1%, cash also has to be ready before the first payroll cycle. The readiness signal is staffed first-client schedules, completed files, and documented training.
Build The Roster Before You Open
Start by matching each client commitment to named caregivers, backup shifts, and payroll timing. If you can’t show who works which hour, and who covers a call-out, you’re not ready to open. That gap usually leads to missed visits, rushed training, and a weak first impression with families and referral sources.
Clear every hire before assignment.
Document background checks and files.
Train for each service role.
Map backup coverage by shift.
Test payroll before first visit.
Keep the first schedule tight and realistic. A staffed calendar with backups is better than a full pipeline with no coverage. That is what protects day-one operations, keeps visit quality steady, and supports referral confidence when the first clients start.
4
Referral And Payer Channels
Referral and payer channels
For disability care, referrals need to start before approval is finished, but you should not convert leads until service fit and staffing are clear. The launch risk is simple: if case managers, waiver coordinators, and family decision-makers can’t get a fast, compliant answer, your first-client pipeline stalls and opening day turns into waiting mode.
The core inputs are a referral list, intake script, eligibility checklist, response-time target, and follow-up workflow. With a $25,000 Year 1 marketing budget and a $750 CAC assumption, the plan supports about 33 clients if every dollar turns into paid starts. Weak proof of compliance or slow follow-up will push that number down fast.
Build the referral handoff
Start outreach to case managers, Medicaid waiver referrals, waiver coordinators, social workers, discharge planners, advocacy groups, schools transitioning adults, and private-pay families before launch, but use a hard gate for conversion. That gate should confirm service scope, eligibility, and live staffing so you don’t promise care you can’t deliver on day one.
Set a response target, then test it. A slow reply after referral intake can cost the first account and damage trust with payers and partners. Keep proof of compliance ready in the first call, because these buyers want to see that documentation, screening, and service boundaries are already in place.
Use one intake script.
Check eligibility before scheduling.
Track every referral within 24 hours.
Assign follow-up to one owner.
Keep compliance proof easy to send.
5
Operations, Billing, And Launch Control
Intake-to-Cash Readiness
Open only when scheduling, visit notes, billing, and payroll all connect cleanly. In disability care, the risk is simple: care gets delivered, but it is not billed cleanly, so cash comes in late and staff pay runs ahead of collections. Day-one readiness means the first client visit can move from intake to service record to claim or invoice without a manual patch.
The fixed admin stack is already a real cost base: $1,000 per month for client management software, $1,800 for liability and workers comp insurance, and $600 for regulatory compliance and licensing. Add 2% payment processing fees on revenue. So the launch test is not just software installed; it’s a working path for client records, HIPAA-aware notes where relevant, certificates, and performance tracking.
Test the first visit before the first visit
Run a full mock cycle: intake, schedule, visit documentation, invoice or claim, payroll, and closeout. If any field is missing, fix it before opening. One clean handoff beats three good intentions. Use a single owner for the workflow and make them verify forms, login access, certificate storage, and billing rules against the exact service scope you plan to deliver.
Test intake-to-payment end to end
Confirm payroll and billing dates
Store client records in one system
Track notes before claims go out
Check compliance files before launch
What this setup protects is speed: faster cash collection, fewer rework loops, and fewer service misses. If documentation or billing steps take too long, day-one operations slow down and your team spends time fixing records instead of serving clients.