 Time to Open6 monthsLaunch runway
Time to Open6 monthsLaunch runwayHow to Open an ECMO Specialist Training Program in 3–9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsLaunch runway  Launch Sequence6 stagesCurriculum first
Launch Sequence6 stagesCurriculum first Key BottleneckStaffing gapLab readiness
Key BottleneckStaffing gapLab readiness First Revenue StepPaid contractCohort booking
First Revenue StepPaid contractCohort booking


To open an ECMO specialist training program, define the learner audience, build an Extracorporeal Life Support Organization (ELSO)-aligned curriculum, secure expert faculty, set up simulation capability, review education approvals, and enroll a pilot cohort Most launches take 3 to 9 months, mainly driven by simulation equipment, instructor availability, and any continuing education approval path The researched planning model assumes 18 billable days per month, 55% Year 1 occupancy, and $2112M Year 1 revenue The first revenue step is usually a paid hospital group cohort, individual clinician enrollment, or an on-site training event
Time to Open6 monthsLaunch runwayLaunch Sequence6 stagesCurriculum firstKey BottleneckStaffing gapLab readinessFirst Revenue StepPaid contractCohort bookingLaunch timeline
This short web summary shows the launch sequence, and the XLSX export contains the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10
Compliance / setup
- Entity filing
- Insurance bind
- Accreditation map
- Director appointment
Curriculum design
- Course outline
- Skills checklist
- Assessment build
- Final syllabus
Faculty hiring
- Director onboarding
- Instructor recruiting
- Technician hiring
- Dry run prep
Simulation lab
- Rent signed
- Buildout kickoff
- Simulator install
- Safety checks
Vendors / IT
- ECMO quotes
- Circuit order
- IT setup
- Mobile unit plan
- Acceptance test
Marketing / enrollment
- Lead list
- Outreach launch
- Hospital sales
- Cohort booking
- First cohort prep
Why test the ECMO Specialist Training Program model before launch?
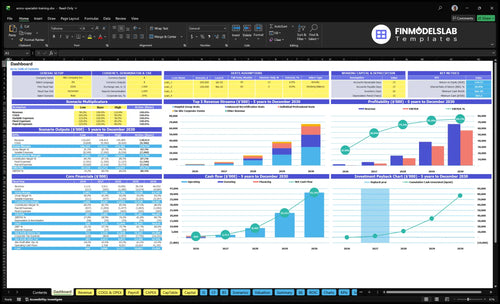
The dashboard in ECMO Specialist Training Program Financial Model Template shows revenue, costs, cash needs, assumptions, and break-even logic—open the model.
Financial model highlights
- $2.112M Year 1 revenue
- $587k Year 1 EBITDA
- 18 billable days monthly
- 55% occupancy assumption
- $503k minimum cash
What do you need to open an ECMO training program?
You need business registration, state education clearance, qualified faculty, medical director oversight, liability coverage, privacy controls, and ELSO-aligned competencies before enrolling learners in an ECMO Specialist Training Program; this How To Launch ECMO Specialist Training Program? guide should be checked against state rules, learner type, certificate claims, and CE or CME plans. The Extracorporeal Life Support Organization registry includes 200,000+ ECMO runs, so hospitals will expect serious clinical governance, not a light skills course.
Launch requirements
- Register the business entity first
- Confirm state education rules
- Set CE or CME path
- Carry professional liability insurance
Clinical controls
- Use credentialed ECMO faculty
- Name a medical director
- Protect patient data under HIPAA
- Align skills with ELSO standards
How do you get students for an ECMO training program?
If you want students for the ECMO Specialist Training Program, start with hospital education departments, ICU leaders, ECMO coordinators, perfusion teams, respiratory therapy managers, nursing educators, and workforce development buyers. Build the first offer around a paid hospital group contract, clinician cohort enrollment, or an on-site training event, and use How To Write A Business Plan For ECMO Specialist Training Program? to frame the pitch. A simple Year 1 mix is 40 hospital group seats at $2,500, 20 individual seats at $3,500, 10 advanced recertification seats at $1,200, and 2 on-site events at $15,000, or $212,000 total.
First buyers
- Hospital education departments first
- ICU leaders and ECMO coordinators
- Perfusion and respiratory therapy managers
- Nursing educators and workforce buyers
Revenue plan
- Sell 40 hospital seats at $2,500
- Sell 20 cohort seats at $3,500
- Sell 10 recert seats at $1,200
- Book 2 events at $15,000
How long does it take to start an ECMO training program?
An ECMO Specialist Training Program usually takes 3 to 9 months to launch. A shorter launch works with rented simulation space, existing faculty, and a narrow pilot cohort; a longer one needs lab buildout, CE approval, vendor lead times, hospital review, and broader competency validation.
Fast launch path
- 3 to 4 months is realistic for a pilot.
- Use rented simulation space first.
- Keep faculty already in place.
- Limit enrollment to a small cohort.
What pushes it longer
- Months 1 to 6: simulators drive the schedule.
- Months 1 to 3: ECMO circuits can bottleneck timing.
- Months 1 to 4: buildout adds delay.
- Months 3 to 8: mobile simulation can stretch setup.
Confirm what must be ready before accepting ECMO students or hospital clients
Launch readiness checklist
Use this go-live approval checklist to confirm the program is ready before opening.
Regulatory
- Entity and tax setupCritical
The program needs a valid legal setup before contracts, billing, and permits move ahead.
- State authorization clearedCritical
Training claims need state approval before you sell seats or issue certificates.
- CE/CME pathway confirmedHigh
If credits are offered, the approval path must be clear before marketing starts.
- Privacy controls enabledCritical
Patient data and trainee records need controls before any case material is used.
Clinical
- Medical director appointedCritical
Clinical oversight must be named before the first cohort and assessment signoff.
- Faculty credentials verifiedCritical
Faculty need documented ECMO experience and active credentials before teaching.
- Competency standards approvedHigh
The program needs a clear pass bar so certificates mean the same thing every time.
- Contract templates reviewedHigh
Participant, hospital, and faculty terms should be locked before any seat is sold.
Curriculum
- Curriculum finalizedCritical
The launch needs one approved learning path with no open gaps in content.
- Simulation scenarios testedCritical
Scenarios should work in practice, not just on paper, before trainees arrive.
- Assessment rubric approvedHigh
A shared rubric keeps grading fair and cuts disputes over competency results.
- Deidentified cases readyHigh
Case material must be deidentified before it can be shown in class or online.
Facility
- Simulation lab builtCritical
The room must be ready for teaching, movement, storage, and cleanup before launch.
- ECMO equipment installedCritical
Core equipment has to be installed and working before any hands-on session starts.
- Consumables stockedHigh
Training supplies need enough stock for the first cohorts and dry runs.
- Mobile unit testedMedium
If on-site events are sold, the transport setup must work before hospital visits.
Systems
- LMS liveHigh
The learning platform must be live so trainees can access content and records.
- Registration workflow testedHigh
If sign-up breaks, the first sales cycle stalls before any class can fill.
- Payment flow confirmedCritical
Billing must collect seats, deposits, and invoices without manual workarounds.
- Recordkeeping workflow setHigh
Completion, assessment, and certificate records need a clean audit trail from day one.
Launch
- Hospital outreach readyCritical
Without a referral path, the program may open with no clear source of trainees.
- Runway covers Month 6Critical
Cash must cover the early dip, since minimum cash lands in Month 6.
- Launch signoff completeCritical
Final signoff should confirm faculty, lab, insurance, enrollment, and assessment are live.
Want to see the six launch drivers that decide opening readiness?
1Curriculum Framework
Scope gateA clear scope, scenarios, and checklist let you take deposits without refund or credential disputes.
2Faculty Oversight
5 rolesLocked medical leadership before marketing keeps cohorts credible and avoids schedule slips.
3Simulation Lab
3-8 moTested simulators and stocked consumables keep opening on time; equipment delays push launch.
4Compliance
Approval gateInsurance, disclaimers, and approval rules tighten contracts and cut opening claims risk.
5Hospital Partnerships
70 seatsHospital buyers and early seat sales prove demand and bring the first revenue faster.
6Cohort Operations
55% occRepeatable cohort steps turn clinical readiness into revenue, with 18 billable days, 55% occupancy, and $2.1M Year 1 revenue.
Curriculum and Competency Framework
Curriculum Sign-Off
This launch gate decides whether you can take deposits at all. If the course does not define the learner audience, adult or pediatric scope, learning goals, simulation scenarios, competency checklist, and certificate language, hospitals can reject the offer or dispute the credential after the first cohort.
Use ELSO-aligned content without claiming affiliation unless you have earned it. The curriculum has to match the skills you promise to ICU, respiratory therapy, perfusion, and nursing buyers, or the opening slips and trust drops on day one.
Build the Approval Packet
Lock one clean packet before marketing: 4 gates — faculty review, medical director approval, LMS setup, and assessment rubrics. That gives you a clear sign-off trail and keeps the opening date tied to what can actually be taught and scored.
- Define learner audience first.
- Match scenarios to promised skills.
- Approve certificate wording early.
- Test LMS access before enrollment.
If scenarios do not match the hospital-facing promise, the risk is not just a bad class. You get refund pressure, credential disputes, and rework that can push the first cohort past the planned open date.
1
Faculty and Medical Oversight
Faculty Locked
For an ECMO specialist training program, faculty is the launch gate. Hospitals are buying clinical credibility and safe hands-on teaching, so the program cannot open cleanly without a contracted Medical Director, Clinical Lead Instructor, Simulation Technician, and backup instructors for each cohort date.
The disclosed Year 1 staffing pool totals $725,000 across the Medical Director at $280,000, Clinical Lead Instructor at $165,000, Simulation Technician at $85,000, Director of Sales at $130,000, and Program Coordinator at $65,000. If schedules are not locked before marketing starts, you can overbook seats, miss cohort dates, and lose trust before day one. No faculty, no launch.
Lock Dates Before Selling
Before outreach begins, get written coverage for every cohort: who teaches, who supervises simulation, who covers absences, and which dates are protected on the calendar. Tie each course date to a named lead and a backup, then confirm the staffing plan against the first cohort roster, room use, and simulation lab schedule.
Also document the handoff between sales and operations. If a hospital signs for a class and the instructor calendar shifts, the program can miss its opening window, delay first revenue, and create avoidable refund pressure. Keep the plan simple: signed faculty, locked dates, backup coverage, and capacity by cohort.
- Contract the Medical Director first.
- Confirm instructor dates in writing.
- Assign a backup for every cohort.
- Match staffing to booked seats.
- Freeze marketing until coverage is fixed.
2
Simulation Lab and Equipment
Simulation Lab Readiness
This lab decides whether you can teach on day one. For ECMO (extracorporeal membrane oxygenation), learners need simulators, circuits, pumps, oxygenator demo materials, and cannulation models where used. If any key item is missing, you can’t run a full scenario, so opening slips and early cohorts lose trust.
The disclosed equipment stack totals $615,000: $250,000 high-fidelity patient simulators over Months 1 to 6, $180,000 ECMO circuit equipment over Months 1 to 3, $120,000 facility buildout over Months 1 to 4, and $65,000 mobile simulation transport over Months 3 to 8. The longest lead items can push launch even if the curriculum is done.
Lock the Lab Early
Order the long-lead items first and test them before marketing starts. The readiness check should be tested equipment, stocked consumables, working scenarios, and simulation technician signoff. Also verify maintenance coverage, spare parts, and transport timing before you take deposits or promise cohort dates.
- Confirm vendor lead times in writing.
- Stage full ECMO scenarios end to end.
- Document maintenance and replacement parts.
- Get technician signoff before enrollment.
If the lab can’t run the first scenario without a fix, day-one operations stall. That can force a launch date move, cut seat sales, and strain cash because the equipment spend lands before tuition does. One clean rule: no open date until the room, machines, and training run all pass signoff.
3
Compliance, Approvals, and Insurance
Compliance Gate
This launch gate decides whether you can sell seats without avoidable claims or enrollment disputes. Before opening, confirm state education review, any continuing education (CE) or continuing medical education (CME) path, exact certificate scope, informed disclaimers, patient privacy rules, safety policies, and contracts. If those terms are loose, you can start marketing before the program can defend what it promises.
The cash drag is real: $3,500 a month for professional liability insurance plus $1,200 for accreditation maintenance equals $4,700 in fixed monthly cost. Education approvals vary by state, credit type, and marketing claims, so one weak approval path can delay opening and force rework on contracts, learner language, and launch materials.
Approval Checklist
Build the approval file before marketing. Verify the target learner group, award type, certificate wording, and the claims you can make in ads and proposals. Then match that language to enrollment forms, contracts, and learner handbooks so every document says the same thing. That keeps day-one expectations clean.
Sequence insurance and policy signoff with faculty review, not after it. Lock coverage, privacy rules, and safety policies before taking deposits, then test the enrollment flow against the approved wording. If review runs long, you still open with clear terms and lower opening risk.
4
Hospital Partnerships and Enrollment
Hospital Access and Enrollment
Hospital access is the first proof that this ECMO specialist training program can sell before it scales. If ICU directors, ECMO coordinators, nursing education leaders, respiratory therapy managers, perfusion teams, and workforce development buyers do not move early, you may still open on time, but day-one revenue will be thin and referral proof will be weak.
The Year 1 demand plan depends on 40 hospital group seats, 20 individual professional seats, 10 advanced recertification seats, and 2 on-site corporate events. At the stated prices, that is about $212,000 in gross revenue if fully sold: $100,000 + $70,000 + $12,000 + $30,000. Here’s the quick math: hospital access is not just marketing, it is the first cash signal.
Enrollment Setup
Before opening, verify the buyer list, seat mix, pricing, invoicing flow, and who can approve a purchase inside each hospital system. If a hospital wants a group seat, know the decision chain, contract path, and start date before you promise capacity. That keeps deposits real and stops launch delays from turning into empty class dates.
Build the outreach in this order: target account list, decision-maker map, seat reservation terms, event dates, and follow-up schedule. If early conversations stall, cut back on open slots fast so you do not tie up faculty time, lab time, or cash for seats that are not closed yet.
- 72 sellable units in Year 1
- Track approval owners by hospital
- Lock event dates before outreach
- Confirm invoice and PO timing
- Use closed seats to fund growth
5
Cohort Operations and Revenue Ramp
Cohort Flow Drives Revenue
Cohort ops is what turns a strong class into repeatable cash. If registration, prerequisites, payment collection, learning management system (LMS) access, learner messages, rosters, instructor ratios, certificates, feedback, and next-cohort scheduling are not in place, the first group may start late or need manual fixes. With 18 billable days per month and 55% occupancy in Year 1, the model only works if each cohort opens on time and closes cleanly.
The ramp is material: model revenue rises from $2.112M in Year 1 to $5.611M in Year 2, tied to 20 days and 65% occupancy. What this hides is rework; if the first cohort is hard to repeat, seat fill, cash collection, and instructor planning all slip, and the next launch window gets pushed.
Lock the Repeatable Runbook
Before opening, map the full cohort flow end to end and assign owners for every step. Verify that payment clears before LMS access opens, rosters match instructor ratios, and certificate language is ready before the final session. That keeps day-one delivery tight and reduces manual fire drills when the first cohort hits.
- Test registration to payment.
- Confirm prerequisites before access.
- Load LMS messages and rosters.
- Lock backup instructors early.
- Schedule feedback and next cohort dates.
6
Related Products
- ECMO Specialist Training Program Porter's Five Forces Analysis
- ECMO Specialist Training Program BCG Matrix
- ECMO Specialist Training Program Business Model Canvas
- What Are The 5 Core KPIs For ECMO Specialist Training Program Business?
- ECMO Specialist Training Program Business Plan Template in Pre-Written Word
- How Increase ECMO Specialist Training Program Profits?
- What Are Operating Costs For ECMO Specialist Training Program?
- ECMO Specialist Training Program Startup Costs: Plan Around $12M
- ECMO Specialist Training Program Financial Model Template in Excel
- How Much ECMO Training Program Owners Make: $587K Year 1 EBITDA
- How To Write A Business Plan For ECMO Specialist Training Program?
- ECMO Specialist Training Program Marketing Mix
- ECMO Specialist Training Program Marketing Plan
- ECMO Specialist Training Program Business Proposal
- ECMO Specialist Training Program PESTEL Analysis
- ECMO Specialist Training Program Pitch Deck Example Editable PPTX
- ECMO Specialist Training Program Business SWOT Analysis
- ECMO Specialist Training Program Value Proposition Canvas
Frequently Asked Questions
Start with the learner type, then build the curriculum, faculty plan, simulation setup, compliance review, and first cohort offer Use the 3 to 9 month launch range as the planning window The model assumes 18 billable days per month, 55% Year 1 occupancy, and $2112M Year 1 revenue