How to Open a Hemodialysis Center: 9–18 Month Launch Roadmap
To open a hemodialysis center in the United States, confirm state licensing and certificate-of-need rules, secure a compliant site, design the treatment area, install dialysis and water systems, hire the clinical team, pass licensure and CMS survey steps, enroll payers, and start treating referred end-stage renal disease patients A realistic dialysis center launch timeline is 9 to 18 months, and it can run longer in certificate-of-need states or complex medical buildouts The key bottleneck is usually licensure/CMS survey readiness plus water system validation In the researched model, the launch plan starts with 6 hemodialysis machines, 6 recliner chairs, 3 registered nurses, 4 dialysis technicians, 1 nephrologist, and a Year 1 utilization assumption of 60%
Time to Open9-18 monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckLicense gateWater readinessFirst Revenue StepTreat referralsClaims ready
Hemodialysis launch timeline
Short web summary of the launch plan; the XLSX export holds the full Gantt Chart.
A Hemodialysis Center usually takes 9 to 18 months to open, and it can take longer if certificate-of-need review, lease delays, water-system redesign, equipment lead times, or survey scheduling slip. The critical path is regulatory confirmation, site control, facility buildout, water system validation, equipment installation, staffing, payer enrollment, survey readiness, referral pipeline, and first treatment scheduling. In a 6-machine, 6-chair setup, about $250,000 for buildout and $150,000 for water purification are not side tasks; sequencing them drives the opening date.
What sets the clock
9 to 18 months is practical.
CON review can add time.
Water system changes slow buildout.
Survey slips push opening back.
What drives the date
Confirm regulatory approval first.
Lock the site and lease terms.
Install and validate water treatment.
Finish payer enrollment before scheduling.
How do dialysis centers get patients?
Hemodialysis Center patients usually come through compliant referral relationships, not broad consumer ads, and revenue only starts after licensure, CMS certification, payer enrollment, and claims workflows are ready. If you want the startup-cost side, see What Is The Estimated Cost To Open And Launch A Hemodialysis Center?; the ramp assumes 60% Year 1 utilization at about $380 per treatment, so referral volume must match chair count and staffing. Build trust with nephrologists, hospital discharge planners, chronic kidney disease care teams, care coordinators, and payers, plus handle eligibility checks, transportation, records intake, scheduling, and continuity-of-care handoffs.
Referral sources
Nephrologists drive early volume.
Discharge planners send post-hospital starts.
Care teams need clear criteria.
Transportation keeps chairs filled.
Readiness first
Licensure comes before first claims.
CMS certification and payer enrollment matter.
60% Year 1 utilization is the plan.
$380 per treatment needs tight staffing.
What licenses are needed to open a dialysis center?
To open a Hemodialysis Center, verify state dialysis facility licensure, Certificate of Need review where required, local zoning/building/fire/health/occupancy approvals, and CMS ESRD certification under 42 CFR Part 494; this is a state-by-state checklist, not legal advice. Build survey readiness around the operating metric covered in What Is The Main Metric That Reflects The Success Of Hemodialysis Center?, because CMS certification depends on documented care, safety, water quality, and quality reporting.
Verify First
State dialysis facility license
Certificate of Need, if applicable
Zoning, building, fire, occupancy approvals
CMS ESRD certification: 42 CFR Part 494
Avoid Bottlenecks
Engage one of 18 ESRD Networks
Validate water before patient treatments
Prepare policies during buildout
Fix incomplete state or CMS files
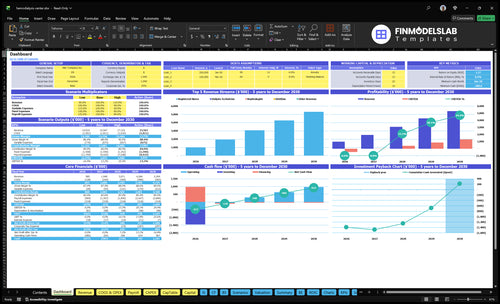
Hemodialysis Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before first patient treatments
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the center is ready for launch.
1Licensing
State licensure approvedCritical
Launch can't start without the state license in hand.
Certificate-of-need clearedCritical
Need this if the state requires a CON before dialysis services open.
CMS Conditions for Coverage metCritical
This is the main federal survey gate for Medicare participation.
ESRD Network requirements confirmedHigh
The network must be aligned before opening patients to care.
2Facility
Building and health approvals clearedCritical
Use this to prove the site passed local build-out and health review.
Water purification validatedCritical
Dialysis water must pass testing before any patient treatment.
Emergency generator testedHigh
Backup power protects treatments when utility power drops.
3Equipment
Dialysis machines installed and testedCritical
All 6 machines must work before the first session.
Treatment chairs installedHigh
Patients need 6 ready chairs for opening day capacity.
Initial supplies stockedHigh
Dialyzers, bloodlines, and concentrates must be on hand.
4Staffing
Medical director agreement signedCritical
The nephrologist needs formal oversight duties before launch.
Year 1 team credentialedCritical
Coverage assumes 3 RNs, 4 techs, 1 nephrologist, 1 dietitian, and 1 social worker.
Clinical policies approvedCritical
Include infection control, patient rights, and adverse-event steps.
5Revenue
Payer enrollment completeCritical
Claims can't go out until payers are set up.
Eligibility and referrals testedHigh
Front desk needs a live path from referral to scheduled visit.
EHR claims workflow readyHigh
Charting, coding, and claim submit steps must all work.
6Finance
Cash runway covers Month 25Critical
Model shows minimum cash near -$589k before breakeven in Month 25.
Open only after compliance, staff, systems, and cash all clear.
Which launch drivers decide the opening date?
1Regulatory Pathway
Licensure gate
The center cannot open without state licensure, certification, and survey-ready files.
2Facility Buildout
Water-ready
Buildout and water treatment must pass inspection before patients can be treated safely.
3Clinical Staffing
3 RNs, 4 techs
Signed oversight and credentialed staff decide whether approved capacity can run on day one.
4Equipment Supply
6 machines, 6 chairs
Installed machines and supply checks keep chair time open after survey approval.
5Billing Readiness
$380/treat
Payer enrollment and clean claims turn each treatment into collectible cash.
6Referral Intake
60% Y1 util
Referral flow must support 60% in Year 1 without outrunning staffing.
Regulatory Pathway
Regulatory Clearance
The center cannot open on time without state licensure, certificate-of-need clearance where required, and CMS certification. For a hemodialysis center, this is the gate, not a checkbox. If the licensing file is incomplete, the opening slips and the first treatment date moves too.
Readiness means the file is complete, policies match state rules, staff records are trained and signed, water logs are validated, emergency procedures are documented, and the survey binder is ready. One clean rule: don’t sign a lease or lock a layout until state-specific requirements are confirmed.
Build the survey file first
Start with a state rule check, local approvals, ESRD Network coordination, and a Conditions for Coverage gap review. Then run a mock survey and fix every gap before filing or scheduling inspection steps. That sequence lowers rework and keeps the launch path realistic.
Assign one owner to track licensure, payer certification alignment, and the corrective-action process. Use a simple launch list:
Confirm state rules before lease signing
Collect local approvals early
Test survey binder completeness
Train staff before inspection
Close every mock survey gap
1
Facility Buildout And Water Treatment
Facility Buildout and Water Treatment
A hemodialysis center cannot open on time unless the site is ready for treatment stations, infection control, patient flow, and water treatment. This is not cosmetic space work; it is the gate that decides whether the clinic can safely treat patients on day one. The researched setup includes $250,000 for facility buildout and $150,000 for the water purification system, plus 6 machines and 6 recliner chairs.
Here’s the quick math: if the water system, plumbing, electrical capacity, emergency access, or waste handling slips, the opening date slips with it. The readiness signal is installed and tested water treatment, documented water quality logs, working treatment stations, emergency power and process plans, clean supply flow, and final inspections. Water is a launch gate, not a setup task.
Sequence Water and Buildout First
Start with design review, then contractor coordination, equipment rough-ins, water testing, biomedical checks, and final inspections. The site needs space for storage, clean and dirty flow, and safe patient movement before the first treatment chair is used. If the layout is wrong, you can pass paperwork and still miss opening because the room cannot support clinical work.
Track these inputs before scheduling a first patient:
$400,000 core setup budget
6 machines and 6 chairs
Water quality logs ready
Emergency power plan tested
Plumbing and electrical signed off
Waste handling path documented
If the water system is treated like equipment delivery instead of a launch gate, opening gets delayed and day-one capacity drops.
2
Clinical Leadership And Staffing
Clinical Staffing Readiness
A hemodialysis center can’t open on time if the right clinicians are not already cleared to work. The Year 1 team needs 1 center manager, 3 registered nurses, 4 dialysis technicians, 1 nephrologist, 1 dietitian, 1 social worker, 1 front desk admin assistant, and 5 medical records clerks; if a licensed role is missing, the schedule and patient flow break on day one.
The readiness signal is signed medical director oversight plus verified credentials, staff competency records, coverage schedules, emergency training, and patient-to-staff workflows. That supports safer ramp-up and fewer survey findings. If hiring slips in a tight clinical labor market, opening may need to move or start below planned capacity.
Hire, Credential, and Drill Early
Start hiring and credential checks before buildout ends. Lock the medical director, nursing coverage, and backup shifts first, then train the team on clinical policy, charting, emergency response, and mock treatment workflows before live patients arrive.
Use this launch check:
Verify licenses and references.
Document competency before scheduling.
Map coverage for every shift.
Test backup staffing for callouts.
Assign workflow owners for handoffs.
3
Equipment And Supply Chain
Equipment and Supply Readiness
This driver decides whether the center can treat patients on day one. If machines, chairs, consumables, and service plans are late, the license may be in hand but the treatment floor still can’t open on time.
The planned setup is 6 hemodialysis machines at $300,000, 6 patient recliner chairs at $30,000, and a $150,000 water purification system. That is $480,000 before buildout, starting inventory, and service contracts. Missing dialyzers, bloodlines, or biomedical support after survey approval can stop first treatments fast.
Lock Vendor and Reorder Rules Early
Confirm vendor contracts, delivery timing, acceptance testing, and backup suppliers before the schedule is fixed. The readiness signal is not just installed equipment; it is a working system for service, storage, and replenishment.
Stock dialyzers, bloodlines, concentrates.
Set par levels and reorder triggers.
Schedule preventive maintenance.
Stage cleaning and emergency supplies.
Train staff on setup and swaps.
One missed consumable can cut chair use for the day, and a weak maintenance plan can turn approved capacity into idle equipment. That hurts opening timing, patient flow, and early revenue.
4
Payer Enrollment And Billing Readiness
Payer Enrollment And Billing
For a hemodialysis center, a treatment slot is not usable cash until the claim is collectible. That means Medicare certification, payer enrollment, and payer contracts where needed must be finished before opening, or the clinic can start treating patients and still wait on payment. With a $380 Year 1 treatment price, day-one billing control matters.
Readiness also depends on eligibility checks, coding setup, claims workflow, denial tracking, and billing system integration. The risk is clear: if the center treats before payer approval, it creates avoidable cash drag, extra rework, and delayed reimbursement even when clinical care is ready.
Build the revenue cycle before the first chair fills
Verify payer files, a tested claim path, patient financial intake, coding review, and cash-posting procedures before opening day. Assign one owner for the revenue cycle, then test the handoff from eligibility to claim submission to denial follow-up so nothing stalls after treatment.
Submit payer applications early
Set up Medicare billing
Test eligibility before treatment
Document denial tracking rules
Confirm EHR integration works
The model assumes 3% for medical billing services and 2% for electronic health record software licenses, so billing setup is part of launch cost, not back-office cleanup. If claims are not clean on day one, the center can be open clinically but short on cash.
5
Referral Network And Patient Intake
Referral Intake Pipeline
A dialysis center does not open safely on day one without real patient flow. With expected utilization starting at 60% in Year 1 and rising to 85% by Year 5, the launch plan has to secure referred patients before the first chair is live, not after. Trust-based referral ties with nephrologists, hospitals, discharge planners, chronic kidney disease practices, care coordinators, and payers are the operating line between a licensed site and a usable clinic.
The hidden risk is passing survey but not having a practical intake path. If record transfer, insurance checks, chair scheduling, transportation, patient education, and continuity-of-care handoff are not mapped, treatment slots stay empty and staff time gets wasted. Here’s the quick math: a 6-chair center at 60% utilization needs a steady intake engine, not generic marketing.
Build the Intake Workflow First
Before opening, verify that every referral source knows the admission path, who sends records, who clears insurance, and who books the first chair. Put the steps in writing: referral meeting, admission checklist, scheduling rules, follow-up timing, and claims readiness. That keeps first-day operations from depending on one person’s memory.
Confirm compliant referral relationships.
Test medical record transfer timing.
Assign insurance verification ownership.
Set transportation coordination rules.
Train staff on handoff scripts.
Track source-by-source intake volume.
What this estimate hides is timing. If referrals lag after launch, staffing still runs, chairs still sit open, and cash needs rise fast. So the intake workflow has to be tested before opening day, with real contact names, real handoffs, and a clear backup plan for slow referral months.
Start by confirming state licensure, certificate-of-need rules, and CMS certification requirements before signing a lease Then validate the site, design treatment stations, plan the water system, and build a staffing model The researched base case uses 6 machines, 6 chairs, 3 registered nurses, 4 dialysis technicians, and 60% Year 1 utilization
A typical launch takes 9 to 18 months The timeline stretches when certificate-of-need review applies, buildout is complex, water treatment needs redesign, hiring slips, or the CMS survey is delayed Treat licensing, buildout, water validation, payer enrollment, and referral development as parallel workstreams with clear go/no-go checkpoints
You generally need CMS certification for an ESRD facility before Medicare-covered treatments can be billed Also verify state licensure and local approvals Certification readiness depends on policies, trained staff, infection control, emergency procedures, water testing, and survey files Opening clinically and billing cleanly are separate readiness tests
The biggest delays are regulatory review, medical buildout, water system validation, equipment delivery, clinical hiring, survey scheduling, and payer credentialing In the researched setup, the buildout is planned around 6 machines, 6 chairs, and a dedicated water purification system If water logs or staff competency records are incomplete, opening should pause
First revenue starts when approved referred patients receive treatments and the claims process is ready Build compliant referral paths with nephrologists, hospitals, discharge planners, care coordinators, and payers At $380 per treatment and 60% Year 1 utilization, the model only works if scheduling, eligibility checks, documentation, and billing happen before the first treatment day
About the author
Jonathan Bell
First-Time Founder Guide Writer
Jonathan Bell is a Financial Models Lab writer focused on launch budget planning, helping aspiring small business owners estimate startup needs before opening. As a first-time founder guide writer, he explains business costs in simple language and offers simple launch planning insights that help readers compare business opportunities realistically and make grounded real-world decisions.
Choosing a selection results in a full page refresh.