Hemodialysis Center Startup Costs: $975K Launch Budget
This dialysis center startup cost breakdown uses researched planning assumptions, not vendor quotes or guaranteed budgets It covers a $975k startup outlay across Month 1 to Month 7, including $950k of hard CAPEX and $25k of initial medical supply stock, plus separate working-capital needs tied to a -$589k minimum cash position in Month 25 The model shows -$479k EBITDA in the first year and breakeven at Month 25, so the funding plan has to carry the early ramp-up period
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a hemodialysis center, before opening and before any working capital needs.
!
CAPEX only This calculator excludes opening inventory, working capital, payroll runway, payer lag, debt service, deposits, and operating losses. It covers hard startup assets only, so use a separate model for post-opening cash needs.
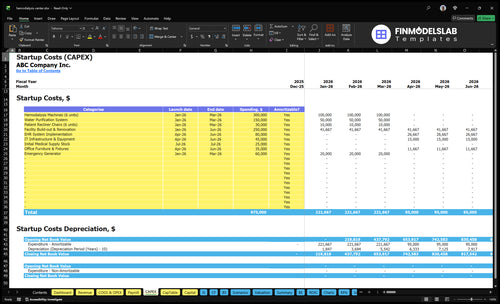
What does the CAPEX tab show?
The Hemodialysis Center Financial Model TemplateCAPEX tab tracks startup costs, timing, depreciation, amortization, and runway. First-year EBITDA is -$479k. Review assumptions.
Financial model screenshot highlights
Machines $300k, buildout $250k
Months 1-7, $265k overhead
Month 25 breakeven, -$589k cash
Hemodialysis Center Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
How much money do you need to open a dialysis center?
You need about $1.56M to open a Hemodialysis Center in this base case, not just the $975k startup list. Equipment alone is not the budget; see What Is The Main Metric That Reflects The Success Of Hemodialysis Center? because cash drops to -$589k in Month 25 and breakeven also lands in Month 25. Here’s the quick math: $975k startup cost + $589k working capital gap = about $1.56M, before contingency, financing fees, deposits, and state-specific regulatory costs.
Base startup budget
$300k hemodialysis machines
$250k clinical buildout
$150k water purification
$25k initial medical supplies
Funding gap drivers
$950k hard CAPEX
$80k EHR implementation
$60k generator
-$479k first-year EBITDA
What is the most expensive part of opening a dialysis center?
The most expensive part of a Hemodialysis Center is usually the regulated facility around the machines, not the machines alone. Here’s the quick math: the listed startup items add up to about $915,000, with $300,000 for hemodialysis machines, $250,000 for buildout, $150,000 for water purification, and $60,000 for an emergency generator. Water and infrastructure matter because dialysis needs reliable reverse osmosis water, plumbing, drainage, electrical capacity, and backup power.
Top cost drivers
$300,000 hemodialysis machines
$250,000 facility buildout
$150,000 water purification
$60,000 emergency generator
What changes the bill
$30,000 treatment chairs
$80,000 EHR implementation
$45,000 IT infrastructure
Station count and patient flow
How should a dialysis center business plan show startup costs?
A Hemodialysis Center business plan should break startup costs into CAPEX, pre-opening, inventory, staffing ramp, payer collections, and cash runway, not a flat checklist. Use the $975k launch outlay, $380 treatment price, 600% first-year capacity, -$479k Year 1 EBITDA, $265k monthly overhead, $699k payroll, and Month 25 breakeven to tie spend to the operating model. Show tabs for depreciation, amortization, reimbursement timing, payer mix, 30% medical billing, and the -$589k cash trough so the runway need is clear.
Startup cost buckets
CAPEX: build and equipment
Pre-opening: licenses and setup
Inventory: launch supplies and meds
Staffing ramp: payroll before full load
Operating link
$975k launch outlay to fund
$265k monthly overhead to cover
-$479k Year 1 EBITDA planned
-$589k cash trough to reserve for
Calculate Fuding Needs
Startup cost summary table
This table summarizes hemodialysis center startup CAPEX and excluded working capital needs across low, base, and high cases.
Highlighted CAPEX$950,000Base planning example
Excluded cash needs$589,000Outside CAPEX total
Funding need$1,539,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Hemodialysis Machines (6 units)
$300,000
Dialysis machine count and equipment spec
Yes
Facility Build-out & Renovation
$250,000
Room build, plumbing, and clinical layout
Yes
Water Purification System
$150,000
Purification capacity and installation scope
Yes
EHR System Implementation
$80,000
Software setup, integration, and training
Yes
Clinical Support Equipment, Furnishings & Backup Power
$170,000
Chairs, IT gear, office furniture, and generator
Yes
Working Capital Reserve
$589,000
Modeled cash trough, payroll timing, and overhead before breakeven
No
Hemodialysis Center Core Five Startup Costs
Facility Buildout and Leasehold Improvements Startup Expense
Buildout Base Case
A dialysis center buildout is often the biggest opening cost. The base case here is $250k from Month 1 to Month 6 for treatment rooms, patient flow, handwashing and infection control, plumbing, drainage, electrical capacity, flooring, HVAC, Americans with Disabilities Act access, staff space, storage, and utility rooms.
What Drives Cost
This is the money that turns a shell into a clinical space. To estimate it, you need square footage, prior medical use, number of treatment bays, whether heavy plumbing already exists, and the landlord work letter. Local code, permits, backup power connections, and water room requirements can move the quote fast.
Ask for a bay count.
Check prior medical use.
Confirm plumbing already exists.
How to Keep It Tighter
Use an existing medical shell if you can, because that cuts demo, plumbing, and permit work. The biggest mistakes are assuming office space will fit dialysis needs and underpricing utility upgrades. One clean rule: if the layout does not support water, power, and infection control, the cheap lease can become the expensive build.
Key Layout Costs
The cost rises with more stations because each bay adds plumbing, drainage, electrical load, and floor area. Backup power and water room needs can add another layer of spend. Landlord approval, local code, and the existing shell condition often matter as much as the finish level.
Dialysis Equipment and Treatment Station Startup Expense
Base case
For a 6-station opening, the source base case shows $300k for hemodialysis machines and $30k for recliner chairs. That is $330k before monitors, scales, emergency gear, carts, installation, service contracts, spare capacity, and biomedical testing. The clean read is simple: machine count sets the cash need.
Per station
Here’s the quick math: $300k ÷ 6 = $50k per machine and $30k ÷ 6 = $5k per chair, so the known base is $55k per station, or $330k total. Use station count, treatment volume, and backup-machine policy to size the order. If the vendor bundles installation or service, keep those quotes separate so the CAPEX stays clean.
Quote the gaps
Do not bury the extras. Ask for separate quotes on station monitors, scales, emergency equipment, carts, installation, maintenance contracts, and biomedical testing. Also confirm whether each machine is new or refurbished; price and service terms change, but this source set gives no discount assumption. One clean quote per line item keeps the budget auditable.
Timing matters
Put the spend in the right month: order timing, delivery, and install dates drive when cash leaves and when stations can open. If the backup machine policy requires spare capacity, add it now, not after launch. The budget should tie to station count, treatment volume, and vendor service terms so the opening-day setup matches clinical flow.
Water Treatment and Dialysis Infrastructure Startup Expense
Water System
A dialysis center can’t treat water as a small line item. The base case sets $150k from Month 1 to Month 3 for reverse osmosis, softeners, carbon tanks, pre-treatment, storage and distribution loops, drain systems, testing, alarms, and backup support. That spend protects patient safety, survey readiness, and machine uptime.
Cost Drivers
Price depends on municipal water quality, loop design, station count, redundancy, and service contract terms. Build the estimate from vendor quotes for the water room, piping, alarms, and testing gear, then tie it to the 6 treatment stations in the equipment plan. More stations and more backup raise the total.
Keep It Tight
Do not cut the water room to save cash. The safer move is to right-size redundancy to the local supply and use any existing landlord plumbing, since heavy utility work can reduce scope. Water, power, and drainage should be planned together with the $250k buildout and $60k emergency generator.
Scope Check
Before you lock pricing, ask for water quality results, municipal supply details, loop design, station count, and backup rules. If the site needs new drains or a full service loop, the water system becomes a schedule risk too, not just a cost item.
Licensing, Certification, and Professional Services Startup Expense
Licensing Path
This line covers the paperwork and expert help needed before the first treatment: state licensing, Centers for Medicare & Medicaid Services (CMS)End-Stage Renal Disease (ESRD) certification, survey prep, payer enrollment, and medical director agreements. Keep it separate from buildout because rules vary by state and payer mix. If approval slips, opening-month cash burn rises before reimbursement starts.
Budget Inputs
Budget it from quotes for legal review, credentialing, consultant support, inspections, policies and procedures, and compliance documentation. Add the months of coverage you need for survey prep and payer enrollment. One clean rule: if the facility is built but not billable, this cost is now a timing problem, not just a paperwork line.
Quote legal and consultant hours
Map payer enrollment timing
Check state certificate rules
Cut Rework
Use one experienced consultant, lock the medical director agreement early, and start payer enrollment before final inspections. The usual mistake is waiting until construction is done, then racing to fix policies and credentials. One clean rule: front-load the compliance work, or you pay for idle space.
Start survey prep early
Track document owners
Avoid last-minute policy edits
Open on Time
Tie this spend to your go-live date, not the lease date. If survey readiness or payer enrollment slips, rent, payroll, and utilities start first while treatment revenue stays at zero. Put the line item in the opening budget so you can see when reimbursement is ready.
Pre-Opening Staffing, Training, and Supplies Startup Expense
Pre-open payroll
Plan for 17 roles in Year 1: 1 center manager, 3 registered nurses, 4 dialysis technicians, 1 nephrologist, 1 dietitian, 1 social worker, 1 front desk admin assistant, and 5 medical records clerks. The source case puts first-year payroll at about $839k, so staffing is one of the largest opening cash needs.
Training and setup
Use pre-opening labor for recruiting, onboarding, competency training, policies, medical director arrangements, and billing setup. This cost is not just wages; it also covers the time needed to get staff ready before the first treatment. Keep it separate from post-launch payroll so you can see true opening burn.
Train before first patient.
Document every competency.
Set billing before launch.
Initial supplies
Budget $25k in Month 7 for opening stock, separate from ongoing consumables after launch. This covers dialyzers, bloodlines, concentrates, medications, personal protective equipment, and linens. The clean way to estimate it is one opening order plus short coverage for start-up volume.
Buy only launch stock.
Track usage by item.
Keep recurring orders separate.
Control opening cash
Here’s the quick math: $839k in Year 1 payroll plus $25k of initial supplies means the staffing-and-stock line alone is about $864k before rent, equipment, or compliance work. The main risk is mixing one-time launch items with ongoing costs. Keep pre-opening labor, startup stock, and recurring software in separate lines.
Compare 3 Startup Cost Scenarios
Startup cost scenarios
A smaller dialysis center can launch with less cash if it trims nonessential items, but the clinical core still drives most of the spend. Larger builds need more stations, water capacity, and staff.
Lean, base, and full launch cases for a dialysis center.
Scenario
Lean LaunchLower Risk
Base LaunchBaseline Risk
Full LaunchScale Risk
Launch model
This keeps station count user-adjustable and funds the clinical core first.
This is the researched 6-station baseline with $975,000 of startup capex.
This adds stations, a larger water system, heavier buildout, and a bigger early cash need.
Typical setup
Smaller square footage, lighter buildout, and phased nonessential furniture lower the opening cash load, but regulatory readiness stays in scope.
It assumes 6 machines, 6 chairs, 60% Year 1 capacity, and a $380 treatment price.
It also needs a stronger staffing ramp and more square footage to support the larger footprint.
Cost drivers
Station count
machines
chairs
buildout
compliance
Water system
buildout
machines
chairs
staffing
More stations
larger water system
heavier buildout
staffing ramp
cash cushion
Planning rangeCAPEX only
Below base caseLean Spend
$975,000Base Spend
Above base caseGrowth Spend
Best fit
Best for founders who want a tighter first launch and can defer noncritical spend without cutting compliance.
Best for founders with patient capital and runway for a 25-month breakeven.
Best for backed teams that can fund a bigger footprint and wait longer for scale to show through.
!
Planning note: These ranges are researched planning assumptions for early planning, not exact vendor quotes or bid prices.
This researched base case needs about $975k before working-capital reserves That includes $300k for 6 hemodialysis machines, $150k for water purification, and $250k for facility buildout The bigger funding plan should also cover the modeled -$589k cash trough in Month 25, so equipment cost alone is not enough
This model reaches breakeven in Month 25 The early ramp is costly because first-year EBITDA is -$479k and Year 2 EBITDA is still -$23k The model improves after volume builds, with EBITDA rising to $408k in Year 3, $855k in Year 4, and $1294M in Year 5
Yes, the staffing plan includes a nephrologist from Year 1 The researched model uses 1 nephrologist in Year 1 and Year 2, then 2 in Year 3 and Year 4, and 3 in Year 5 It also includes registered nurses, dialysis technicians, a dietitian, a social worker, and administrative staff
Fund the buildout, equipment, opening stock, and operating runway as separate buckets The base startup list is $975k, but the model also shows a -$589k minimum cash position and Month 25 breakeven That points to a planning need near $156M before contingency, financing costs, and any state-specific regulatory costs
The source budget includes $25k for initial medical supply stock in Month 7 After opening, Year 1 medical supplies are modeled at 70% of revenue, pharmaceuticals at 60%, billing at 30%, and electronic health record licenses at 20% That means inventory planning should match patient volume, not just station count
About the author
Max Cooper
Founder Support Writer
Max Cooper is a founder support writer at Financial Models Lab, helping local business owners understand how small businesses make a profit. He focuses on practical planning before money is invested, with clear guidance on startup cost estimates and basic business planning. His work helps readers move from an idea to a simple, workable plan with confidence.
Choosing a selection results in a full page refresh.