How to Open a Hyperbaric Oxygen Therapy Clinic in 4-9 Months
Hyperbaric Oxygen Therapy Clinic
To open a hyperbaric oxygen therapy clinic, choose the service model, confirm state medical requirements, secure qualified clinical oversight, lease compliant space, order FDA-cleared chambers, set up oxygen and fire-safety systems, train staff, build referral demand, and open with controlled first treatments A researched planning range is 4-9 months, with the main bottleneck usually being chamber installation plus oxygen and fire marshal approval In the Year 1 model, staffing starts with 1 hyperbaric physician, 2 HBOT technologists, 1 registered nurse, and 1 patient coordinator First revenue should come from a paid clinical evaluation or physician-referred treatment plan scheduled before the full public launch
Time to Open6 monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckApproval gateFire and oxygenFirst Revenue StepPaid evalIntake ready
Launch timeline
This is a short web summary of the launch plan, and the XLSX export includes the detailed Gantt Chart.
For a Hyperbaric Oxygen Therapy Clinic, plan on 4-9 months to open. The fastest path needs a clean lease, room layout approval, chamber order lead time, oxygen setup, fire marshal review, trained staff, and booked referral consults. If chamber size, ventilation, electrical load, oxygen storage, or emergency steps are fixed after the lease, the schedule usually slips.
Fastest path
Lease and room plan first
Order chamber early
Confirm oxygen vendor availability
Book referral consults now
Delay risks
Wrong chamber dimensions
Late ventilation changes
Electrical upgrades after lease
Fire safety signoff stalls
How do you get patients for an HBOT clinic?
Start before opening: build physician referrals, wound-care and recovery ties, local SEO, and booked consults so you have referral-ready demand at soft opening, not broad ads after chambers arrive. For the launch-budget side, see What Is The Estimated Cost To Open And Launch Your Hyperbaric Oxygen Therapy Clinic?; the Year 1 model assumes 620 monthly treatments and marketing plus patient acquisition at 5% of revenue.
Build demand first
Target physician referral paths first
Partner with wound-care teams
Use local SEO for condition searches
Pre-book educational consults
Keep it compliant
Screen patients before scheduling
Use qualified clinical evaluation
Avoid unsupported treatment claims
Match marketing to medical conditions
Do you need a license to open an HBOT clinic?
Yes, a Hyperbaric Oxygen Therapy Clinic usually needs state-level approvals before opening, but the exact license depends on the state, service model, and whether treatments are medical or wellness-focused; verify this before signing a lease or buying chambers. Start with medical oversight, facility permits, oxygen approval, and fire review, then compare patient experience benchmarks like What Is The Current Customer Satisfaction Level For Hyperbaric Oxygen Therapy Clinic? before launch.
Must Check
Confirm state healthcare facility rules
Appoint a qualified medical director
Clear oxygen storage and delivery
Pass fire and life-safety review
Risk Points
FDA-cleared HBOT uses cover 13 conditions
Track consent forms and patient records
Document emergency protocols before opening
Get healthcare counsel early; permission can block launch
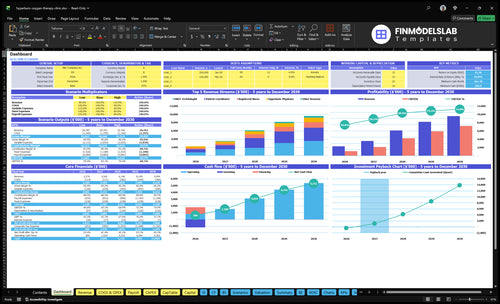
Hyperbaric Oxygen Therapy Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm the clinic is ready before treating patients
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
1Regulatory
Legal entity formedCritical
A formed entity is needed before contracts, permits, and payer setup can move forward.
Healthcare counsel review completeCritical
Counsel should confirm state and facility rules before any patient care starts.
Supervising physician assignedCritical
A qualified physician must be named before launch and escalation decisions.
2Safety
Fire approval receivedCritical
Fire clearance is a hard gate for opening a pressurized treatment room.
Emergency shutoffs testedCritical
Shutoffs must work fast so staff can respond to chamber or oxygen issues.
Safety drills completedHigh
Drills prove the team can handle fire, power loss, and patient escalation.
3Equipment
FDA-cleared chamber documentedCritical
The chamber source should be documented before purchase, install, and use.
Medical oxygen vendor securedCritical
A steady oxygen supply is essential or the clinic cannot run treatments.
Monitoring equipment installedHigh
Monitoring gear must be ready before the first patient enters the chamber.
4Staff
Year 1 headcount coveredCritical
Year 1 needs 1 physician, 2 technologists, 1 nurse, and 1 coordinator.
Chamber operators trainedCritical
Operators must know chamber use, monitoring, and basic patient handling.
Intake and consent readyCritical
Consent and intake forms must be ready before the first scheduled visit.
5Revenue
Billing workflow testedHigh
Billing has to work before launch so cash collection does not stall.
Payment processing testedHigh
Card and payment setup must clear cleanly before the first patient pays.
Referral outreach activeHigh
Referrals need to start early or the clinic will open without demand.
6Finance
Cash at month 6 coveredCritical
The model shows minimum cash of $166k in Month 6, so runway must cover that dip.
Model assumptions still fitHigh
Year 1 staffing and volume should still fit the plan before go-live.
Go-live signoff approvedCritical
Do not open until fire approval, protocols, training, consent, and oxygen supply are complete.
Which launch drivers decide opening-day readiness?
1Medical Governance
Compliance gate
Assigned physician and compliant protocols cut shutdown risk and keep first treatments clean.
2Chamber Setup
4-9 mo
Chamber specs and room layout must be locked before lease or build-out, or installation slips.
3Life Safety
Safety gate
Fire marshal and oxygen approvals can delay opening, so safety plans should land before installation.
4Staffing Flow
Year 1 team
Year 1 staffing of 1 physician, 2 technologists, 1 nurse, and 1 coordinator supports safe flow.
5Referral Pipeline
5% rev
Pre-booked referrals and compliant outreach help the clinic ramp faster after chambers go live.
6Utilization Ramp
620/mo
Scheduling and chamber hours turn capacity into cash, with 620 monthly treatments in Year 1.
Medical Governance And Compliance
Medical Governance and Compliance
For an HBOT clinic, compliance is not cleanup after the lease is signed; it is a launch gate. You need a named medical director or qualified supervising clinician, plus written screening rules, treatment protocols, emergency escalation, consent, and documentation standards before the first patient is booked. If those pieces are late, opening slips and first treatments carry higher shutdown and billing risk.
This is also state-specific, so the same plan can pass in one state and stall in another. Marketing claims must match approved clinical review, not hopeful wording, or referral conversations get messy fast. Done right, the clinic starts safer, documents cleanly, and avoids avoidable charting gaps from day one.
Lock the clinical rule set first
Verify the supervising clinician is assigned, credentials are current, and scope-of-practice matches state rules before you schedule patients. Then approve the intake screen, consent form, treatment protocol, emergency escalation plan, and chart template. If any of those are still being drafted when booking opens, the launch plan is too loose.
Match marketing to approved review.
Use one documentation standard.
Train staff on escalation steps.
Recheck state facility requirements.
Keep referral language conservative.
What this hides: weak compliance can delay opening even when the room and chamber are ready, because the clinic still cannot safely or legally treat the first patient.
1
Chamber Procurement And Room Layout
Chamber Procurement
If the FDA-cleared chamber type is not selected early, the room plan can drift, and that pushes back the physical opening date. This driver matters because the chamber sets the room dimensions, electrical load, ventilation needs, and maintenance access before construction is locked.
The launch risk is simple: when chamber delivery, installation, and room approval run on separate timelines, you get redesigns and slow signoff. Manufacturer training should be booked before soft opening so staff can use the chamber on day one, not after the first patient is waiting.
Map The Room First
Get the chamber specs before you sign a lease or finalize construction. Here’s the quick math: if the room is wrong, you pay twice, once to build it and again to fix it. Verify clearances, patient flow, and service access on the same drawing set, so the install team, clinician, and contractor are working from one plan.
Confirm chamber model and cut sheet.
Match room size to equipment clearance.
Map power and ventilation early.
Protect maintenance access on all sides.
Schedule manufacturer training before opening.
What this hides: a bad layout can delay installation signoff even when the chamber has arrived. Lock the equipment plan first, then align construction, room approval, and staff training to the same opening date.
2
Oxygen, Fire, And Life-Safety Approvals
Fire and Oxygen Approval Path
For a hyperbaric oxygen therapy clinic, fire safety is often the launch bottleneck. The oxygen delivery or storage plan, fire marshal review, emergency shutoffs, chamber safety rules, and staff response drills all have to match the building and the local authority before installation, or the first-treatment date slips.
Here’s the real risk: if oxygen storage conflicts with the lease or building rules, the clinic can be built but still not open. That means more idle rent, more equipment sitting in place, and more pressure on staffing and referral timing. Safe day-one care depends on getting the life-safety signoff right, not fixing it after the chamber arrives.
Verify the Life-Safety Plan Early
Start with the oxygen plan, then get the fire marshal and building team aligned on storage, shutoffs, signage, and suppression needs. The clinic should also document chamber safety protocols, emergency steps, and staff roles so the opening checklist matches what inspectors expect.
Confirm oxygen storage location first.
Map shutoffs and emergency access.
Review signage and suppression rules.
Train staff on response procedures.
Coordinate with local authority early.
If the site requires a different oxygen setup than the one planned, treat that as a schedule risk right away. Fixing it after equipment is ordered can push installation, delay inspection, and leave the clinic open on paper but not ready to treat patients.
3
Staffing, Training, And Clinical Workflow
Safe Day-One Staffing
Year 1 staffing has to fit the treatment flow, not just the org chart: 1 hyperbaric physician, 2 HBOT technologists, 1 registered nurse, and 1 patient coordinator. This is what lets the clinic open on time and run controlled first treatments with clear monitoring, intake, and scheduling coverage.
If the team is short on chamber operators or intake support, the first week gets messy fast. That raises no-show risk, slows room turnover, and puts extra load on the supervising clinician. A w ellness coach waits until Year 2; opening day should stay focused on medical oversight and safe workflow.
Train Before You Book Volume
Before opening, confirm manufacturer or approved equipment training, safety drills, monitoring steps, and who covers each handoff. The readiness signal is simple: every role knows intake, chamber setup, patient monitoring, emergency escalation, and closing tasks before the first appointment is booked.
Assign one owner for intake.
Train chamber operators first.
Document opening-day roles.
Test scheduling and no-show steps.
Run a safety drill before soft open.
What this setup prevents is wasted chair time and last-minute confusion. When the RN, technologists, and coordinator are trained as one flow, the supervising physician can stay focused on oversight instead of putting out fires.
4
Referral Demand And Patient Pipeline
Referral Pipeline Ready
A hyperbaric oxygen therapy clinic can’t wait until chambers are live to start demand. The readiness signal is simple: local SEO is set, a referral list is built, physician and specialist outreach is underway, approved education materials are in hand, and screening rules are ready so every lead gets checked against qualified use. That keeps marketing aligned with medical approval and avoids launch-day gaps.
Year 1 plans set marketing and patient acquisition at 5% of revenue, so this is a controlled spend, not a blank check. Start early and the clinic can ramp faster toward 620 monthly treatments; start late and you add cash drag after opening because the rooms are ready before the calendar is. One clean rule: no lead moves forward without screening.
Pre-Book Before Open
Build the pipeline before the first treatment day. Confirm the referral list, publish compliant pages, and book evaluation visits on the calendar so the opening week already has qualified patients. Keep claims tight and evidence-based; avoid unsupported promises and route every inquiry through a documented review process.
Track three launch checks: pre-booked evaluations, referral outreach, and screening approval. If one slips, first-day volume slips too. That shows up fast in a fee-for-service clinic, because empty slots on day one become lost revenue and slower payback on the launch spend.
Set SEO before chambers arrive.
Train referral scripts on approved uses.
Log every lead to screening.
Book evaluations before opening.
5
Scheduling, Utilization, And Revenue Ramp
Scheduling, Utilization, And Revenue Ramp
HBOT clinics turn clinical readiness into cash only if the schedule can convert booked patients into completed treatments. The Year 1 plan assumes 60%-65% capacity and 620 monthly treatments, which is about 21 treatments a day; if treatment length, chamber hours, or staffing coverage are off, opening can slip or first-day volume can collapse.
Here’s the quick math: 120 × $450, 160 × $350, 140 × $300, and 200 × $500 totals $252,000 a month. With 12% direct and variable costs, contribution is about $221,760 before fixed overhead and payroll, so the launch only works if no-show policy, payer or cash-pay workflow, and booking rules are already tight.
Test the calendar before opening
Build the opening schedule around treatment length, chamber hours, packages, and staffing coverage, then test it against the 620-treatment ramp. If the day falls apart when one patient cancels, the model is too thin for day-one operation.
Start by choosing the clinical service model, confirming state requirements, and securing qualified medical oversight Then lease space that fits chamber, oxygen, electrical, ventilation, and fire-safety needs The researched opening range is 4-9 months, and the Year 1 staffing model starts with 1 physician, 2 technologists, 1 nurse, and 1 patient coordinator
Plan on 4-9 months, not a fixed date The timeline depends on lease approval, chamber procurement, oxygen setup, fire marshal review, staff training, and referral demand If chamber specs or oxygen storage rules are checked late, the buildout can stall even when the medical team is ready
Plan for physician or qualified clinical oversight before launch Requirements vary by state and service model, but HBOT involves patient screening, treatment protocols, monitoring, documentation, consent, and emergency escalation Treat medical governance as an opening dependency, and verify ownership, supervision, and scope-of-practice rules with healthcare counsel
The common delays are chamber delivery, room layout conflicts, oxygen infrastructure, fire-safety approval, and staff training The biggest avoidable error is buying chambers before confirming site fit Build the timeline around safety signoff, because first treatments should not start until equipment, protocols, and trained operators are ready
The first revenue step is a paid clinical evaluation or physician-referred treatment plan scheduled before the full launch Use pre-opening outreach to book qualified consults, not to promise outcomes In the Year 1 model, revenue depends on 620 monthly treatments and 60%-65% capacity, so referral readiness matters early
About the author
Matthew Clarke
Founder Support Writer
Matthew Clarke is a founder support writer at Financial Models Lab, where he helps non-finance readers understand practical profit planning and how small businesses make a profit. He focuses on clear, research-based guidance before money is invested, including startup cost estimates and early planning basics. His work makes business planning easier, more practical, and less intimidating.
Choosing a selection results in a full page refresh.