To start a medical practice in the United States, you need licensed providers, a legal entity, National Provider Identifier setup, malpractice coverage, payer enrollment, Health Insurance Portability and Accountability Act policies, Occupational Safety and Health Administration basics, a ready facility, working electronic health record and billing systems, trained staff, and booked patients A researched planning range is 4–9 months, with payer credentialing and buildout usually driving the opening date In this model, buildout runs through Month 5, electronic health record implementation runs Month 3 to Month 4, and first revenue depends on booked visits with an active payment path The financial check matters because the model’s minimum cash need is $670,000 in Month 5, even though breakeven is modeled in Month 2
Time to Open4-9 monthsLaunch runwayLaunch Sequence8 stagesCompliance firstKey BottleneckCredentialing gateProvider enrollmentFirst Revenue StepBooked visitsPayment path live
Clinic launch timeline
This is a short web summary of the clinic launch plan; the XLSX export includes the detailed Gantt Chart.
What licenses do you need to open a medical practice?
You’ll need provider medical licenses from the state medical board first; this is not legal advice, but it’s the gate before a Medical Practice can enroll with payers, open the facility, and see patients. Align the checklist with What Is The Main Goal You Aim To Achieve With Your Medical Practice?, because Month 1 compliance already includes $3,300/month: $2,500 malpractice insurance plus $800 general liability.
License first
State medical board provider licenses
Business entity setup
Internal Revenue Service Employer Identification Number
National Provider Identifier for billing
Go-live checks
State registrations and local permits
Drug Enforcement Administration registration if needed
How do you get patients for a new medical practice?
You get patients for a new Medical Practice by driving first billable visits, not just awareness: build local search visibility, appointment pages, insurance directory listings, referral ties, community outreach, launch announcements, and fast scheduling, plus use How Much Does It Cost To Open And Launch Your Medical Practice Clinic? to keep launch costs aligned. In Year 1, plan for 30% of revenue to go to patient referral and acquisition, with $1,000/month for marketing and the website. New revenue only lands after eligibility checks, intake forms, coding, claims submission, payment collection, and payment posting, so demand has to match capacity.
Get booked visits
Show up in local search.
Use direct appointment pages.
List every insurance directory.
Build referral ties weekly.
Protect cash flow
Set aside 30% for acquisition.
Keep marketing at $1,000/month.
Run eligibility before each visit.
Match demand to Year 1 capacity assumptions: 650% for primary care physicians, 600% for nurse practitioners, 700% for medical assistants.
What are the biggest mistakes when opening a medical practice?
The biggest mistakes when opening a Medical Practice are moving too fast on the lease, opening before credentialing and payer enrollment are done, and starting with weak billing and front-desk setup. One model still needed $670,000 in cash in Month 5 even with Month 2 breakeven, so timing gaps can hurt fast. The fix is simple: set go-live gates for payer status, claim testing, staff scripts, intake forms, equipment readiness, insurance verification, and runway.
Main risks
Don’t sign the lease too early
Don’t open before credentialing
Don’t delay marketing until launch
Don’t skip billing setup
Go-live gates
Confirm payer status first
Test claims before opening
Train front desk scripts
Verify cash runway monthly
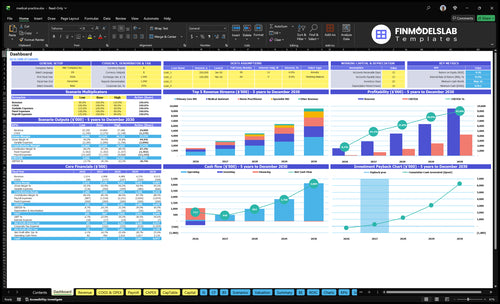
Medical Practice Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before seeing patients
Launch readiness checklist
Use this go-live approval checklist before opening a medical practice.
1Licensing
State board and license verifiedCritical
You can't see patients until the clinic and clinicians are licensed.
Entity, EIN, and NPI setCritical
Billing and payer setup need a legal entity, tax ID, and provider ID.
Malpractice and liability policies boundCritical
Coverage should be active before the first patient or staff shift.
DEA registration confirmedHigh
Needed if the practice will prescribe controlled substances.
2Facility
Clinic lease, buildout, and access approvedCritical
The space must be usable before staff, patients, and vendors arrive.
Exam rooms and equipment installedCritical
Rooms need working furniture, diagnostic tools, and supplies.
Utilities, waste, and cleaning liveHigh
Power, waste pickup, and cleaning support safe daily operations.
3Clinical systems
EHR and scheduling liveCritical
The team needs a working record and booking flow on day one.
Intake and eligibility workflow testedHigh
This avoids delays at check-in and reduces bad billing data.
HIPAA and OSHA basics trainedHigh
Staff must know privacy, safety, sharps, and exposure rules.
4Revenue cycle
Booking and payment flow testedCritical
Patients need a clear path from booking to payment without friction.
Billing workflow and clearinghouse readyCritical
Claims must move cleanly or cash will lag after launch.
Payer enrollment and coding liveCritical
Without payer setup, the practice may treat patients but not collect.
Payment posting and denial pathHigh
You need a fast way to post cash and fix denied claims.
5Staffing
Year 1 staff hiredCritical
Year 1 assumes 2 primary care MDs, 1 NP, 2 MAs, 1 manager, and 1 front desk.
Credentialing and privileges approvedCritical
Providers need payers and facility access approved before seeing patients.
Front desk and rooming trainedHigh
Strong rooming cuts wait time and keeps visits moving.
6Finance
Runway covers opening cash needsCritical
The model's minimum cash is $670k in Month 5, so runway must cover that dip.
Fixed costs and wage load checkedCritical
Rent, payroll, insurance, and software must fit the first-year plan.
Go-live signoff completedCritical
This confirms compliance, staffing, systems, and cash are ready.
Want to review the six main medical practice launch drivers?
1Payer Credentialing
4-9 mo gate
Active enrollment and payer contracts decide when booked visits can bill and cash can start.
2Clinical Compliance
License gate
Licenses, privacy rules, and insurance coverage must be live before care starts, or shutdown risk rises.
3Facility Readiness
M1-M5 build
Month 1 to Month 5 buildout must finish before patient visits can begin.
4EHR Billing
M3-M4 EHR
Month 3 to Month 4 EHR setup shortens billing lag and speeds first claims.
5Staffing Workflows
Year 1 team
Year 1 staffing of 2 physicians, 1 nurse practitioner, 2 medical assistants, 1 manager, and 1 front desk keeps visits moving.
6Patient Acquisition
$670K M5
Marketing works only after credentialing and scheduling are live, or cash burns before revenue.
Payer Credentialing And Provider Enrollment
Provider Enrollment Before Day One
Payer credentialing is usually the longest gate before insured patients can be seen and billed. Until the practice has active provider enrollment, payer contracts, fee schedules, directory listings, and eligibility checks live, booked visits can turn into unpaid visits. That slows first revenue and can create avoidable denials in the first operating month.
This step includes National Provider Identifier setup, payer applications, contracting, enrollment tracking, and claim test planning. If marketing starts before plans are billable, demand can outrun cash collection. The real readiness test is simple: a patient can book, verify coverage, be seen, and move into a live payment path.
Enroll, Test, Then Open
Work the sequence in order: assign NPI, submit payer files, track approvals, load fee schedules, confirm directory data, and test eligibility plus claims before the first appointment. One clean check now is worth weeks of cash pain later.
Match contracts to target plans.
Verify each payer status weekly.
Test a sample claim flow.
Hold launch ads until billing is live.
1
Clinical Compliance And Licensing
Licensing Before First Patient
Patient care cannot start until the practice has licensed providers, state registrations, and the right policies in place. If any of those are late, the opening slips, staff sit idle, and the first visit can create avoidable shutdown risk. The launch also starts with $2,500 per month for malpractice insurance and $800 per month for general liability, so the clinic is carrying $3,300 per month before day one revenue.
Here’s the quick math: compliance is not a back-office task here; it is the gate. The practice needs HIPAA privacy policies, OSHA basics, incident workflows, records retention, consent forms, and prescribing registration if needed. If staff training is weak, the clinic may open late or open unsafe, which hurts patient trust and raises the chance of a regulatory stop.
Verify and document before opening
Work the checklist in order: state medical board checks, provider licenses, state registrations, insurance binders, privacy policies, and safety procedures. Do not schedule the first patient until each item has a named owner and a dated proof file. One missing approval can block the whole front door.
Confirm provider licenses first.
File HIPAA and consent documents.
Train staff on incidents and records.
Test prescribing registration, if needed.
Archive insurance and policy evidence.
The real launch risk is not paperwork by itself. It is opening without a clean compliance trail, because that can delay patient care, slow staffing, and force a pause after the first week. Keep the file ready before the schedule goes live, so day-one operations are legal, safe, and stable.
2
Medical Office Setup And Clinic Buildout
Clinic Buildout
Care cannot start until the space is ready, so the buildout path sets the opening date. Here the hard spend is about $328,000 across Month 1 to Month 5, with $150,000 for renovation, $40,000 for exam room furnishings, and $75,000 for diagnostic equipment. If the lease, inspections, utilities, access, or equipment delivery slip, patient-ready capacity slips too.
The real risk is opening a shell instead of a clinic. Exam rooms, IT, waiting area furniture, security, office equipment, cleaning, waste handling, and staff training all have to land before the first visit. One clean line: no ready rooms, no open doors. A late inspection or delayed equipment install can push revenue and force more preopening cash burn.
Buildout Checklist
Sequence the work in the order that protects the opening date: lease control first, then permits and inspections, then construction, then furnishings, equipment, and systems. The model already ties key items to the first 3 to 5 months, so treat vendor lead times as critical path items, not side tasks. Don’t schedule patient launch until the room, power, network, and cleaning plan are all tested.
Before opening day, verify these inputs are live:
Lease signed and access confirmed
Inspection dates locked
Equipment delivery scheduled
Waste handling vendor in place
Staff training completed
IT and security tested
3
EHR Setup And Medical Billing Workflow
EHR and Billing Go-Live
For a medical practice, this is the point where care turns into cash. The first revenue readiness signal is live scheduling, intake, eligibility, documentation, coding, clearinghouse, claims submission, payment posting, denial tracking, and reporting. If this chain is not live, you can see patients but still stall collections.
Here’s the quick math: the model carries $2,000 per month for EHR and scheduling software, plus a $25,000 EHR implementation from Month 3 to Month 4. Year 1 billing and collections service fees run at 60% of revenue, so weak setup quickly turns into slow cash and more denials. The big risk is opening before claims can move.
Go-Live Setup Check
Before opening, verify the billing path end to end: payer enrollment, trained front office staff, clean patient intake, and a test claim flow. If any step is missing, the practice may have visits on the schedule but no clean way to bill them. That creates billing lag and pushes cash collection out.
Confirm payer enrollment status.
Test eligibility before first visit.
Train staff on coding handoffs.
Run denial and posting workflows.
Document who owns each step, when the EHR goes live, and what gets tested before day one. The goal is simple: one patient visit should flow from check-in to claim submission without manual rework.
4
Medical Practice Staffing And Workflows
Day-One Staffing Match
Staffing has to match day-one patient volume, or the clinic opens with bottlenecks instead of care. The Year 1 team is 2 primary care physicians, 1 nurse practitioner, 2 medical assistants, 1 practice manager, and 1 front desk staff. Annual wages total $768,000, so the launch plan has to support about $64,000 per month in payroll from the start.
What this covers is hiring, credential files, scheduling templates, triage scripts, rooming, lab handoffs, billing handoffs, and front desk training. If any one of those is late, visits back up, charges get missed, and first appointments feel slow. One weak handoff can turn a full schedule into a messy one.
Build The Workflows Before First Patient
Before opening, assign every step to a named role and test the flow end to end. A clinic can staff the right headcount and still fail on day one if the rooming process, triage script, or billing handoff is unclear. Here’s the quick math: 6 staff roles means 6 sets of tasks that must be ready before the first visit starts.
Hire before template finalization.
Train front desk on first-call intake.
Test rooming and lab handoffs.
Document billing handoffs clearly.
Use a simple go-live check: if a new patient can be booked, roomed, seen, and billed without a manager rescuing the flow, the staffing model is ready. If not, opening on time is still possible, but first-day service will feel rough and collections will slip.
5
Medical Practice Marketing Launch
Marketing That Books Visits
For a medical practice, marketing only helps if it turns into scheduled visits. Day-one readiness means live appointment booking, accurate online listings, insurance directory visibility, and a follow-up flow that converts calls into visits, not loose interest.
Here’s the quick math: fixed marketing and website spend is $1,000 per month, or $12,000 a year, plus patient referral and acquisition costs at 30% of Year 1 revenue. If demand shows up before credentialing or scheduling works, you can burn cash and still miss the opening target.
Launch Only What Can Convert
Build the first-patient plan around active payers and available provider templates. Match launch announcements, referral outreach, and local search pages to the exact appointment slots you can actually open, so incoming demand lands in a bookable calendar.
Before opening, verify the booking path end to end: listings, directory status, insurance checks, and follow-up ownership. One clean rule helps here: if a patient can’t book in one step, the launch is not ready. That keeps marketing from outrunning staffing and billing setup.
Start with licensure, entity setup, National Provider Identifier, malpractice insurance, payer enrollment, facility readiness, and billing setup A solo launch can be leaner than this model, which starts with 2 primary care physicians, 1 nurse practitioner, and 2 medical assistants Still, the same blockers apply: credentialing, EHR setup, staff workflow, and enough cash to cover the opening ramp
Start payer credentialing as early as possible in the launch plan The full opening window is commonly 4–9 months, and credentialing can gate insured visits even if the clinic space is ready In this model, buildout runs Month 1 to Month 5 and EHR implementation runs Month 3 to Month 4, so payer work should run in parallel
Often you need a practice location for payer applications, but do not treat the lease as the only starting point Confirm the sequence with payers, state rules, and advisors before signing long commitments The model starts rent at $12,000 per month in Month 1, so a delayed credentialing path can create cash pressure quickly
The biggest delays are payer credentialing, buildout, EHR implementation, hiring, and missing compliance items This model has renovation through Month 5, diagnostic equipment in Month 2 to Month 3, and EHR implementation in Month 3 to Month 4 If staff training, claims testing, or eligibility checks are not ready, first visits can turn into slow collections
The first step is to build a launch sequence with blockers, owners, and go-live tests Start with provider licensure, entity setup, National Provider Identifier, insurance, payer enrollment, lease assumptions, and cash runway The model shows breakeven in Month 2 but minimum cash of $670,000 in Month 5, so readiness and timing both matter
About the author
Timothy Dawson
Small Business Educator
Timothy Dawson is a small business educator at Financial Models Lab who helps readers understand the numbers behind everyday business ideas, with a focus on pricing, margin basics, and the common business costs that shape early decisions. He writes about the practical choices founders need to make before launch, especially when planning the first months after a business opens and evaluating whether an idea makes sense.
Choosing a selection results in a full page refresh.