You’re launching a clinical service before you’re launching a storefront, so the first job is readiness This midwifery practice launch plan covers licensing, protocols, coverage, systems, referrals, scheduling, billing, and first-client flow, with 3 to 9 months as the practical planning range
Time to Open6 monthsSetup windowLaunch Sequence6 stagesLicensure firstKey BottleneckLicense gateState rulesFirst Revenue StepBillable visitsIntake ready
Launch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt chart.
What happens to cash if opening slips by one month?
A one-month slip adds about $36,733 of cash burn before revenue starts; at capacity, monthly revenue is about $98,250, so runway and break-even move out. See the revenue, costs, cash needs, assumptions, and break-even logic in the Midwifery Practice Financial Model Template. Open the model.
Cash impact highlights
Extra burn: $36.7k
Revenue starts one month later
Break-even moves later
What mistakes cause midwifery practice launch risks?
The biggest launch mistake in a Midwifery Practice is opening before transfer protocols, malpractice coverage, informed consent, backup coverage, documentation, billing, and referral channels are ready. That creates day-one risk, especially if the founder markets services outside state scope or accepts clients without clear transfer criteria. If fixed expenses are $13,400 a month and wages are about $23,333, burn hits $36,733 before the client pipeline is active.
Launch gaps
Set transfer rules before first client
Carry malpractice coverage on day one
Use clear informed consent forms
Match services to state scope
Money and ops
Test the EHR before launch
Set up superbills and claims flow
Screen clients with hard referral criteria
Schedule on-call backup coverage
How long does it take to open a midwifery practice?
Midwifery Practice usually takes 3 to 9 months to open. Faster launches need clean licensure, ready malpractice coverage, a simple care setting, an EHR that’s live, and direct-pay intake. Slower launches usually come from payer credentialing, facility setup, birth-center buildout, or transfer-pathway work, so plan first revenue around eligible prenatal visits or signed care agreements when compliant.
Faster launch drivers
Finish licensure before clients.
Bind malpractice coverage first.
Use a simple care setting.
Set up EHR and intake.
Slower launch drivers
Payer credentialing can slow cash.
Facility setup adds weeks.
Birth-center buildout adds time.
Transfer pathways need alignment.
How do you get clients for a midwifery practice?
You get clients for a Midwifery Practice by building local trust first—start with doulas, OB-GYNs, lactation consultants, childbirth educators, pediatricians, birth groups, labs, imaging providers, and community education partners, then make booking simple. For the cost side, see How Much Does It Cost To Open A Midwifery Practice?; the first revenue step is turning prenatal consults into signed care agreements or billable prenatal visits, and Year 1 should assume 70% lead midwife capacity and 65% staff midwife capacity, not full utilization.
Build local trust
Partner with doulas and OB-GYNs
Meet lactation consultants and educators
Connect with pediatricians and birth groups
Use community talks to build referrals
Convert interest
Set up local search pages
State service scope clearly
Use consultation calls and intake forms
Follow payer rules on every claim
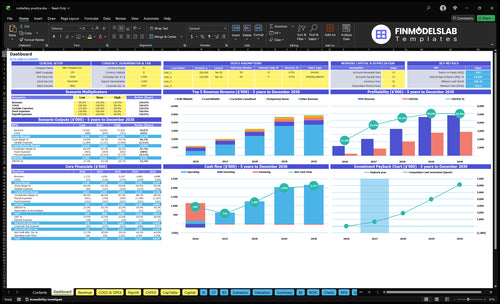
Midwifery Practice Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Build a midwifery practice checklist that prevents day-one failure
Launch readiness checklist
Use this go-live approval checklist before opening the midwifery practice.
1Regulatory
State licensure verifiedCritical
Licensure must be active before any client care starts.
Practice scope approvedCritical
Scope, prescriptive authority, and birth setting rules must be clear.
Malpractice policy boundCritical
Coverage has to be in force before accepting clients.
2Safety
Emergency transfer plan documentedCritical
Transfers need a written path before labor and delivery care begins.
Consent forms approvedHigh
Informed consent lowers risk and keeps client expectations clear.
Charting standards setHigh
Charting must be consistent for care, audits, and incidents.
3Site
Clinic space readyHigh
The space needs privacy, safety, and patient flow ready for care.
Equipment installed and testedCritical
Core equipment must work before the first client visit.
Supply workflow setHigh
Supplies and pharmaceuticals need a simple restock process.
4Systems
HIPAA EHR testedCritical
The EHR must protect PHI and support care documentation.
Booking and intake liveHigh
Clients need a working path to schedule and share history.
Billing flow testedCritical
Claims, superbills, and payment collection must work before launch.
5Staffing
Lead midwife staffedCritical
The model depends on one lead midwife from opening month.
Coverage roster confirmedHigh
Backup coverage reduces gaps in visits, births, and postpartum care.
Team training completeHigh
Staff need the same process for handoffs, escalation, and notes.
6Runway
Cash runway reviewedCritical
Minimum cash hits $795k in Month 2, so runway needs a hard check.
Referral partners confirmedHigh
OB-GYN, hospital, doula, pediatrician, lab, and imaging links drive flow.
First revenue offer readyHigh
The first offer must match client needs and the billing setup.
Go-live signoff completeCritical
Final approval should confirm compliance, care, systems, and cash are ready.
Which six launch drivers matter most before opening?
1State Scope
3-9 mo
State approval sets scope, setting, and collaboration rules, so the practice can open safely on time.
2Care Model
5 roles
A clear care model matches staffing and visit lengths, so intake is safer and pricing is cleaner.
3Risk Mgmt
$2.5K/mo
Coverage and consent rules lower launch risk and make partners more willing to refer clients.
4Referral Net
Transfer plan
Documented transfer partners speed handoffs when care needs rise and keep launch delays lower.
5EHR Billing
HIPAA live
HIPAA-ready charting and billing keep intake, claims, and payments moving without avoidable lag.
6First Clients
Signed care
Signed care agreements and billable prenatal visits turn opening activity into early revenue.
State Licensure And Legal Scope
Licensure and Scope
State rules decide whether a midwifery practice can open on time and serve clients from day one. They control independent practice, where births can happen, what services can be offered, whether collaboration is required, and whether any prescriptive authority applies. If the legal scope does not match the care model, the launch can stall even when staffing and demand are ready.
The readiness signal is written confirmation of credential status, scope, setting, and any supervision or collaboration tasks. Before launch, review the state board, check license renewal timing, align the business entity, confirm payer enrollment fits the license, and review policies. The bottleneck risk is building around services the state does not allow.
Confirm Scope Before You Schedule Births
Lock the legal scope first, then build the service menu. If the practice plans home births, birth center births, hospital attendance, or prescriptions, each item needs state approval in writing. One mismatch can force rework, delay opening, or make early client agreements unusable.
Use a launch checklist that ties the board file, licensure status, payer setup, and policy manual together. Keep a dated record of what the state allows and what it requires. If collaboration is mandatory, set that workflow before taking the first client so day-one care matches the law.
State board scope review
License renewal check
Entity and payer match
Policy and supervision review
1
Care Model And Clinical Protocols
Clinical Scope and Care Path
If the care model is not written before booking starts, the practice can’t open safely on time. The scope has to spell out prenatal visits, labor and birth support, postpartum care, newborn checks, lactation support, childbirth education, risk screening, and transfer criteria, then match staffing, supplies, visit length, scheduling, and client fit.
Year 1 capacity also has to be real, not hopeful. The plan assumes 1 lead midwife at 8 monthly packages and 70% capacity, plus 1 staff midwife at 12 monthly packages and 65% capacity. If the care path is broader than that setup, day-one operations slip, intake gets messy, and unsuitable clients get in before the team can serve them well.
Document the Scope First
Before launch, write the visit map, staff roles, supply list, and transfer rules in one place. That lets the founder price services clearly, screen clients safely, and confirm the practice can handle the first full month without overbooking.
Match visit length to staffing.
Set transfer criteria before intake.
Limit bookings to capacity.
Define newborn and postpartum checks upfront.
Confirm supplies before first visits.
Here’s the quick math: if the team books beyond the stated monthly package load, the practice needs more coverage or a narrower scope. Otherwise, the launch risks late visits, weak follow-up, and rushed care at the exact point when families expect consistency.
2
Malpractice And Risk Management
Malpractice Coverage First
If this midwifery practice books clients before professional liability coverage matches the actual services and birth setting, launch risk jumps fast. The model assumes $2,500 per month for malpractice and liability insurance from Month 1, so coverage is not a later add-on. It is a day-one gate that affects whether the practice can open safely and keep referrals credible.
This launch driver also includes informed consent, emergency policies, documentation standards, incident response, backup coverage, and client risk screening. Weak setup here can delay opening, create compliance gaps, and force awkward last-minute client changes. Strong setup lowers operational risk and helps build trust with payers and partner clinics.
Verify Coverage Before Scheduling
Start with the policy terms, then match them to the exact care plan. Confirm what settings are covered, what services are allowed, and who steps in if the lead midwife is unavailable. That sequence matters because the bottleneck risk is not insurance cost alone; it is accepting clients before the policy fits the work.
Use a short readiness check before opening:
Confirm coverage starts at Month 1
Match terms to birth setting
Document consent and risk screening
Set emergency and incident steps
Line up backup coverage in writing
One gap in that chain can slow first-day operations, confuse referrals, and weaken confidence from partners who expect a clean risk process.
3
Referral And Transfer Network
Referral And Transfer Network
For a midwifery practice, a safe referral and transfer path is part of launch readiness, not a later add-on. If a client needs a higher level of care and there is no documented handoff plan, the practice can open with demand but still fail on day one operations, because care stops where transfer starts.
This network should include OB-GYNs, hospitals, doulas, pediatricians, lactation consultants, labs, imaging providers, and childbirth educators. The launch risk is simple: strong marketing can fill consults, but weak transfer coverage can delay care decisions, slow intake, and hurt trust the first time a client needs escalation.
Document The Handoff Before You Open
Before opening, verify a hospital transfer plan, referral scripts, handoff forms, and clear escalation criteria. Assign who calls, who documents, who sends records, and which cases move out of scope so the first client visit does not depend on improvisation.
Write the transfer steps.
Map each referral contact.
Test urgent-case escalation.
Confirm record-sharing workflow.
Run a mock urgent case before launch. The plan should show how the practice reaches a hospital or specialist, what information goes out, and how the client is guided. If that path is slow or unclear, scheduling may look ready, but clinical operations are not.
4
EHR, Billing, And HIPAA Systems
EHR And Billing Go-Live
EHR and billing are day-one gates, not admin extras. For a midwifery practice, the system has to handle HIPAA-compliant charting, scheduling, telehealth, intake forms, privacy workflows, claims or superbills, and payment collection before the first client walk-in. A usable launch signal is one test client record that moves from consult to chart note to payment or claim submission without gaps.
The monthly software floor in the model is $500 total: $300 for administrative software subscriptions plus $200 for professional licenses and fees. If credentialing is incomplete or documentation is weak, reimbursement can lag and cash gets tight fast. That shows up as slower intake, billing delays, and lost prenatal visits right when the schedule should be filling.
Test The Full Client Flow
Before opening, verify the full path works: consult booking, consent forms, charting, telehealth, coding, invoicing, superbill generation, and claim submission. One clean test record should move through every step with no manual workaround. If a staff member has to patch the process on day one, the launch is not ready.
Assign someone to check credentialing status, form templates, privacy settings, and payment rules before the first appointment. Also confirm that the documentation supports insurance billing, because weak notes can slow reimbursement and force more self-pay collection. That protects launch timing and keeps first-month cash from slipping.
Run one end-to-end test client.
Confirm HIPAA workflows are active.
Check claims and superbill output.
Verify payment collection before launch.
Match documentation to billing rules.
5
First-Client Acquisition And Revenue Ramp
First-Client Ramp
If the practice opens without signed care agreements, day-one capacity sits idle and cash comes in late. For this model, Year 1 monthly revenue at capacity-adjusted volume is about $98,250, with $6,000 birth packages plus smaller lactation, education, and postpartum services. The launch win is earlier signed care agreements and billable prenatal visits, not just website traffic.
Marketing has to stay healthcare-appropriate and match the service scope. If intake is vague, clients book the wrong service, or never convert from consult to care. With marketing and client acquisition at 50% of Year 1 revenue, the implied monthly spend is about $49,125 at the modeled revenue level, so the funnel needs to work before opening day.
Launch-Ready Intake Flow
Build the first-client funnel around local search, referral partners, childbirth education networks, consultation calls, community trust, service packages, and follow-up workflows. The key is to sequence these before opening so each inquiry can move from contact to consult to signed care without delay.
Make the intake path concrete: define which services are offered, what each package includes, and when prenatal visits become billable. Then test the workflow end to end, from first call to booking to follow-up, so the practice can start collecting revenue from day one instead of waiting for the pipeline to catch up.
Start by checking whether your state allows the credential type and birth setting you plan to use Then confirm malpractice coverage, transfer protocols, informed consent, HIPAA-ready charting, and backup coverage A lean home-visit model may fit the 3 to 9 month launch range, but only if licensing and transfer pathways are clear
First revenue can start before the birth month if prenatal consultations convert into signed care agreements or billable prenatal visits The researched model prices birth packages at $6,000 in Year 1 and assumes 70% lead midwife capacity and 65% staff midwife capacity Credentialing delays can push insured revenue later
Not always, but it affects your launch plan A direct-pay practice may open sooner if state rules, malpractice, and documentation are ready If you plan to bill insurance, payer credentialing can become a major delay, so build cash runway around fixed expenses of $13,400 per month plus listed wages
The common delays are state licensure questions, malpractice approval, payer credentialing, EHR setup, clinical protocols, and hospital transfer relationships If any one of these is unfinished, opening gets risky Use the 3 to 9 month range as a planning window, then test intake, billing, and transfer workflows before first clients
Hire when demand, coverage needs, and cash flow support the added schedule The researched plan starts Year 1 with 1 lead midwife and 1 staff midwife, then grows staff midwives to 2 in Year 2 and 3 in Year 3 Don’t hire ahead of protocols, referral flow, or billing readiness
Choosing a selection results in a full page refresh.