Midwifery Practice Startup Costs: $795K First-Year Funding Plan
You’re planning a clinical business before cash collections are proven, so separate assets from launch expenses and runway This outline uses researched planning assumptions for a US midwifery practice with $206,000 in modeled startup asset spending, $13,400 in monthly fixed overhead, and $795,000 in minimum cash for the first operating year Actual midwifery practice opening costs vary by state, practice model, facility type, payer timing, and staffing plan
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a midwifery practice, not payroll runway or other operating funding needs.
!
What this leaves out This tool covers capitalized startup assets only. It excludes payroll runway, working capital, debt service, deposits, malpractice premiums, licenses, and operating spend. The source model also lists website development and initial medical supplies, but those are not included in this pure CAPEX view.
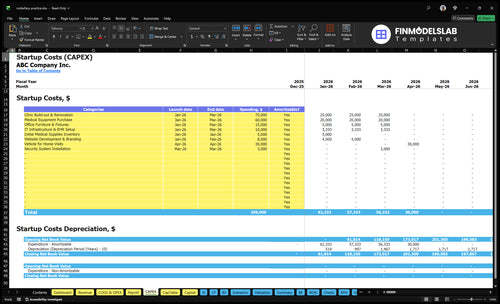
What does this model screenshot validate?
This screenshot in Midwifery Practice Financial Model Template validates CAPEX: $206,000 startup costs, launch timing, depreciation, amortization. Open and adjust assumptions.
Screenshot highlights
$206,000 startup assets
Launch timing by phase
Depreciation and amortization
Working capital and runway
$795,000 minimum cash
$13,400 monthly overhead
$520,000 payroll Year 1
Revenue capacity assumptions
Payer timing matters
Stress test key drivers
Midwifery Practice Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What hidden costs of starting a midwifery practice affect cash runway?
For a Midwifery Practice, the hidden startup costs hit cash runway fast: fixed overhead is about $3,900/month before owner pay, and How Much Does The Owner Of A Midwifery Practice Typically Make? shows why the income side matters early. These costs are mostly timing costs, not long-term assets, so cash leaves now while revenue often lands later. Year 1 variable costs also total 140% of revenue across medical supplies, equipment upkeep, marketing, labs, and referrals.
Monthly cash drain
$2,500 malpractice and liability insurance
$500 property insurance
$200 licenses and fees
$300 admin software
Runway lag
$400 office supplies
Credentialing delays slow collections
Payer enrollment can delay cash
Billing lag and legal review extend runway pressure
Transfer agreements, backup coverage, and supply replenishment add more cash strain before steady pay starts. The practical risk is simple: if revenue is slow, owner draw gets squeezed first.
What makes home birth midwife startup costs different from birth center midwifery startup costs?
Facility choice is the biggest cost driver for a Midwifery Practice: a birth-center-style setup can start with $75,000 in build-out, plus $8,000 monthly rent, $1,000 utilities, $500 maintenance, and $3,000 security installation. A home-birth or mobile model can skip most of that, but it still needs clinical equipment, supplies, insurance, a vehicle, software, and emergency protocols. So don’t mix low-overhead mobile assumptions with birth-center costs.
Home-birth startup costs
Skip clinic build-out.
Skip monthly rent.
Still buy clinical supplies.
Still carry insurance and software.
Birth-center startup costs
Add birth rooms and equipment.
Expect higher utility costs.
Expect bigger coverage needs.
Expect heavier compliance work.
How should founders prepare midwifery practice funding and financial projections?
Midwifery Practice needs a funding plan that covers more than startup assets: use the $795,000 minimum cash need, $206,000 in startup assets, $13,400 in monthly fixed overhead, $520,000 in Year 1 salaries, and a 140% variable cost load to talk to lenders, grant makers, or investors. Here’s the quick math: don’t commit to full staffing until you validate payer timing, because cash flow has to hold while revenue catches up.
Funding proof
Show the $795,000 cash floor.
Separate $206,000 from working cash.
Include $13,400 monthly overhead.
Use loans, grants, self-funding.
Staffing proof
Model 700% lead midwife capacity.
Model 650% staff midwife capacity.
Model 600% lactation and education.
Model 650% postpartum nurse capacity.
Calculate Fuding Needs
Startup Cost Summary
This table summarizes the biggest launch asset costs and the non-CAPEX cash reserve needed to open the practice.
Highlighted CAPEX$190,000Base planning example
Excluded cash needs$795,000Outside CAPEX total
Funding need$985,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinic Build-out and Renovation
$75,000
Leasehold work, clinic fit-out, and room prep
Yes
Medical Equipment Purchase
$60,000
Exam, birth, and clinical care equipment
Yes
Vehicle for Home Visits
$30,000
Transportation for home and postpartum visits
Yes
Office Furniture and Fixtures
$15,000
Waiting area, desks, storage, and seating
Yes
IT Infrastructure and Electronic Health Record Setup
$10,000
Software setup, devices, and clinic systems
Yes
Operating Reserve
$795,000
Covers payroll, rent, taxes, and post-launch cash shortfalls
No
Midwifery Practice Core Five Startup Costs
Facility And Care Setting Startup Expense
Facility setup cost
A clinic model needs $75,000 in build-out plus $8,000 rent, $1,000 utilities, $500 maintenance, and $3,000 security install. That covers lease deposits, exam rooms, waiting space, storage, signage, accessibility, basic safety, and birth rooms if you run a birth-center-style site. Monthly occupancy cost is $9,500 before deposits.
What to include
Use two inputs: one-time build-out and monthly facility run rate. Here’s the quick math: $75,000 upfront plus $9,500 per month in fixed occupancy costs. If the model is mobile home birth, remove rent and most build-out, and the funding need drops fast.
Quote lease deposits first
Price rooms by function
Separate mobile from clinic
How to control it
Keep the space lean at launch. Skip extra square footage, stage the build-out in phases, and don’t add birth-room finishes unless the volume justifies it. The biggest mistake is funding a clinic like a home-visit practice; rent and build-out change the cash need right away.
Phase nonessential rooms later
Negotiate deposits before signing
Match space to visit mix
Clinic or mobile
A fixed clinic carries the $75,000 build-out plus $9,500 monthly occupancy cost, so it needs more startup cash before revenue starts. A mobile home-birth practice avoids most rent and renovation spend, so the funding math is lighter and the early break-even target moves down fast.
Clinical Equipment And Durable Medical Assets Startup Expense
Durable Assets
This block is mostly CAPEX (capital spending), not monthly spend. The durable total is $115,000: $60,000 medical equipment, $15,000 furniture and fixtures, $10,000 IT and EHR setup, and $30,000 for a home-visit vehicle. Keep the separate $5,000 medical supply inventory out unless you track it elsewhere.
What It Covers
Build this estimate from unit counts and vendor quotes. It should cover exam tables, fetal dopplers, blood pressure monitors, scales, sterilization equipment, oxygen setup, emergency equipment, newborn assessment tools, computers, and mobile-care cases. If you offer home visits, the vehicle is part of the same launch block, and room count drives furniture and IT needs.
Count each room and device
Separate clinic and home-care items
Keep disposables in supplies
How To Trim It
Cut costs by phasing purchases, not by cutting safety gear. Compare quotes on furniture, IT, and the vehicle first, since those move the most. Buy used only where it is safe and compliant. If home visits are still light, delay the $30,000 vehicle until demand is clear and keep backup monitoring, oxygen, and sterilization in place.
Phase noncritical purchases
Avoid duplicate devices
Protect core clinical safety
Cash Timing
This spending hits cash before collections start, so it sits next to rent, licensing, and payroll in the launch budget. Here’s the quick check: if quotes for durable assets move above $115,000, re-sequence the build and protect working capital before opening.
Licensing, Credentialing, Insurance, And Compliance Startup Expense
Licenses First
State licensing, entity setup, payer credentialing, and compliance policies can slow launch more than the fee amount suggests. Build this line item from state-specific filing rules, renewal timing, legal review, and transfer or backup agreements. These costs hit cash before the first collection, even when they are not capital assets.
Monthly Cash Drag
Use $2,500 a month for malpractice and liability insurance, $500 for property insurance, and $200 for professional licenses and fees. That is $3,200 in monthly startup cash outflow before any patient revenue lands. One clean number matters here: $3,200.
State Rules Drive Cost
State-by-state rules drive both cost and timing. One state may need faster licensing renewal, while another may slow payer credentialing or require extra compliance policies. Budget for the steps, not just the fees, because the sequence of approvals can delay opening and stretch the startup cash plan.
Cash Before Collections
These are operating costs, not equipment purchases. Even when the practice has no capital asset to show for them, insurance, licenses, credentialing, and compliance still drain cash before collections start. If payer enrollment lags, the practice carries those costs while revenue is still catching up.
Technology, Billing, And Administrative Systems Startup Expense
Startup Stack
Plan $10,000 for IT infrastructure and EHR setup, $300/month for admin software, and $8,000 for website and branding. This block covers EHR, scheduling, patient portal, billing and claims tools, telehealth, secure messaging, phones, laptops, cybersecurity, and HIPAA-related systems. It is setup plus run-rate, not clinic build-out.
What It Covers
Keep this separate from equipment CAPEX. Use vendor quotes for setup fees, user count × monthly price for subscriptions, and months of coverage for launch. The goal is to fund the stack you need on day one, not every tool on the market.
EHR and billing go here
Hardware sits elsewhere
Monthly software is recurring
Trim The Stack
Cut cost by buying one system that handles EHR, scheduling, billing, and portal work instead of separate tools. Avoid paying twice for messaging or telehealth. Keep cybersecurity and HIPAA features in place. The biggest mistake is underfunding training, which slows adoption and creates rework.
Avoid duplicate vendors
Price onboarding first
Lock in support early
Cash Gap
Payer enrollment and claims timing affect working capital because cash can trail launch activity. Budget enough to carry software, support, and admin costs before the first reimbursements land. That timing gap matters more than the software bill itself when you open with a full schedule.
Staffing Readiness, Supplies, And Launch Operations Startup Expense
Payroll Runway
This cost belongs in working capital, meaning cash for day-to-day operations, not CAPEX. The salary plan alone is $520,000 in Year 1, or about $43,333 a month, before supplies and launch spend. Add $5,000 of opening inventory, $400 monthly office supplies, and marketing tied to 50% of Year 1 revenue.
Staff Cost Build
Seven roles total $520,000: lead midwife director $120,000, staff midwife $90,000, lactation consultant $70,000, childbirth educator $60,000, postpartum nurse $75,000, practice manager $65,000, and administrative assistant $40,000. The estimate changes with hiring dates and whether backup coverage is paid or on-call.
Hire to match opening volume.
Price backup coverage upfront.
Keep billing support staffed early.
Launch Consumables
Start with $5,000 of medical supplies inventory and $400 a month in office supplies, or $4,800 a year. Add launch marketing at 50% of Year 1 revenue, lab and referral fees at 30%, and medical supplies and pharmaceuticals at 40%. Model these as cash needs tied to service volume.
Cash Control
Use billing support and a tight start date to bridge the gap between visits and collections. If hiring slips by one month, payroll burn drops by about $43.3k, but care gaps can hurt continuity. A cleaner launch is to stage hires, keep backup coverage ready, and avoid paying full staff before patient flow is real.
Compare 3 Startup Cost Scenarios
Scenario table
Lean, base, and full launches change costs fast here because the model moves from home-based care to an office, then to a larger birth-center setup with more staff and facility spend.
Lean, base, and full midwifery launch costs
Scenario
Lean LaunchAsset-light
Base LaunchBalanced
Full LaunchCapital intensive
Launch model
Home-based and mobile care with no full clinic build-out.
Office-based prenatal and birth support with the modeled core team.
Birth-center-style care with more rooms, more coverage, and heavier compliance load.
Typical setup
Starts with a small core team, home visits, and limited facility needs.
Uses the $206,000 startup asset base, $13,400 monthly fixed overhead, and $520,000 Year 1 salaries.
Adds more staffing depth, more equipment, and higher facility support than the base case.
Cost drivers
Home visits
no full build-out
no clinic rent
lighter utilities
basic equipment
Facility rent
build-out
salaries
malpractice coverage
client acquisition
Larger facility
more equipment
added staff
higher utilities
more insurance and compliance
Planning rangeCAPEX only
Reduced startup cashLowest cash
$795,000 - $1,000,000Core model
Above $1,000,000Highest burn
Best fit
Best for founders with low fixed-cost tolerance and a home-birth focus.
Best for operators who want a standard clinic model and can fund the modeled cash need.
Best for founders aiming at birth-center scale and able to carry higher burn risk.
!
Planning note: Scenario ranges are researched planning assumptions, not exact quotes or vendor bids.
This model holds $795,000 in minimum cash because payroll and facility costs start before cash flow is stable The first operating year includes $520,000 in salaries and $13,400 in fixed monthly overhead If payer enrollment or claims payments lag, that cash cushion protects payroll, insurance, rent, supplies, and backup coverage while patient volume ramps
The model places major setup spending in the startup period, with clinic build-out, medical equipment, furniture, and IT setup running through the first three months The home-visit vehicle is modeled in Month 4 Real timing depends on state licensing, credentialing, facility readiness, payer enrollment, and how quickly you can staff clinical and administrative roles
Yes, plan for malpractice and liability coverage before seeing patients This model budgets $2,500 per month for malpractice and liability insurance, plus $500 per month for property insurance The exact cost varies by state, scope of services, birth setting, claims history, and insurer rules, so treat this as a planning input, not a quote
Buy durable equipment when your care setting and opening timeline are locked This model spends $60,000 on medical equipment, $15,000 on furniture and fixtures, and $10,000 on IT infrastructure and EHR setup during the startup period Delay nonessential extras until patient volume proves demand, but don’t delay emergency, monitoring, or compliance-critical equipment
Usually, yes, because it can reduce facility-heavy costs, but it is not cost-free In this model, the office-based setup includes $75,000 for build-out and $8,000 monthly rent, while mobile care still needs clinical equipment, supplies, insurance, software, and a $30,000 home-visit vehicle The cheaper model still needs working capital for payroll and billing delays
Choosing a selection results in a full page refresh.