How To Open A Mobile Diagnostic Imaging Business In 3 To 6 Months
To open a mobile diagnostic imaging business, you need state-specific compliance review, registered imaging equipment where required, credentialed technologists, physician order workflows, radiologist interpretation coverage, HIPAA-ready operations, billing setup, and signed referral pathways A realistic mobile imaging startup timeline is usually 3 to 6 months, depending on compliance, equipment, vehicle setup, hiring, and payer readiness In the first-year model, X-ray capacity is planned at 65% with 3 techs, while ultrasound capacity is planned at 60% with 2 techs The bottleneck is rarely one task it’s getting compliance, equipment, staff, interpretation, and first facility orders ready at the same time
Time to Open3-6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckLicense gateLead timeFirst Revenue StepReferral ordersOrders live
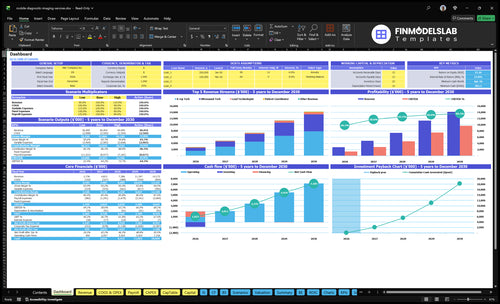
Launch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt chart.
What licenses are needed to start a mobile diagnostic imaging business?
To start Mobile Diagnostic Imaging, you typically need state radiation equipment registration for mobile X-ray, qualified operators, safety records, HIPAA safeguards, insurance, physician-order workflows, radiologist interpretation, and payer credentialing before billing insurance; What Is The Current Growth Trajectory Of Mobile Diagnostic Imaging? matters only after compliance is cleared. Treat this as a launch gate across 50 states, not legal advice, because ultrasound and X-ray rules can differ by modality and location.
Core approvals
Register mobile X-ray equipment where required
Use qualified radiologic operators
Keep quality assurance and safety records
Confirm ultrasound credential and supervision rules
Billing readiness
Require 1 physician order before each exam
Protect patient data under HIPAA
Credential payers before insurance billing
Use CLIA only if lab testing starts
What are the biggest mistakes when starting a mobile diagnostic imaging business?
The biggest mistake in Mobile Diagnostic Imaging is launching before demand, compliance, staffing, interpretation, billing, and routing are tested together. Facility interest alone doesn’t pay the bills; you need signed referral workflows and scheduled studies, or revenue will lag even after you hire the team. A safer start is a soft launch in a tight service area, with 65% X-ray and 60% ultrasound Year 1 capacity assumptions, and denials tracked from day one.
What to test first
Get signed referral workflows first
Book scheduled studies before hiring
Test route density in one area
Track denials from day one
What gets missed
State radiation rules
Equipment quality assurance
Radiologist turnaround protocol
HIPAA and claim setup
How long does it take to start a mobile diagnostic imaging service?
Mobile Diagnostic Imaging usually takes 3 to 6 months to open in the U.S., and the real clock is driven by compliance, equipment, vehicle upfit, hiring, vendor setup, billing, and referral onboarding. Start state review and radiation registration first, because either one can block launch. Even if operations are ready, payer enrollment and billing setup can delay collections, so recruit early for the Year 1 staffing plan of 3 X-ray techs and 2 ultrasound techs.
What can slow it down
State review can stop launch.
Radiation registration comes first.
Payer enrollment can delay cash.
Vendor setup takes real time.
How to move faster
Run tasks in parallel where allowed.
Start equipment procurement early.
Hire before the launch month.
Use a soft launch first.
Key Takeaways
Compliance must clear before the first patient.
Equipment and vehicle testing drive service reliability.
Staffing and workflow set capacity and turnaround.
Runway depends on signed demand and utilization ramp.
Regulatory And Modality Compliance
Regulatory First
Compliance is a launch gate, not admin work. If the state review, technologist credentials, physician order protocol, HIPAA process, and insurance setup are not done, service can stop before the first patient. For X-ray, radiation equipment registration and modality rules add another layer, so the launch path changes by service line.
One missed approval can delay day one. The risk is treating paperwork as a back-office task after marketing starts. That creates a bad sequence: demand is promised before the business can legally or safely deliver. For mobile imaging, the first patient only counts if records, safety steps, and payer readiness are already in place.
Sequence the approvals
Verify the rules before you book visits. Start with state-specific healthcare review, then confirm what applies to each modality. If X-ray is in scope, register the radiation equipment, document safety procedures, and make sure quality assurance logs and records standards are ready. Build the physician order workflow before sales outreach.
Test the full path, not just the forms. Confirm technologist credentials, insurance, HIPAA handling, and the payer credentialing path in the same launch checklist. If ultrasound is the only live modality at first, say so clearly and do not sell X-ray until its requirements are complete. That keeps opening dates real and first-day operations clean.
Confirm state rules by modality.
Register X-ray equipment early.
Document QA and safety logs.
Test HIPAA and records flow.
Verify payer credentialing before launch.
1
Equipment And Vehicle Readiness
Equipment and Vehicle Readiness
If the equipment is not on hand, calibrated, insured, and tested in the vehicle workflow, the business cannot complete paid studies on day one. For mobile imaging, service reliability starts with a working unit, safe transport, and image transfer that actually works before the first visit is booked.
The big dependency is vendor lead time and maintenance access. If ultrasound gear or staffing slips, a limited X-ray-only route can keep the launch moving instead of canceling visits. That protects first-month operations and reduces avoidable downtime while the full setup comes online.
Pre-open Equipment Check
Before opening, lock the scope: X-ray, ultrasound, or both. Then confirm power, storage, vehicle fit-out, infection control supplies, image transfer, and backup plans. Here’s the quick test: if a tech can load, scan, transmit, and leave safely from the vehicle, the setup is close to ready.
Verify calibration and maintenance status.
Confirm insurance is active.
Test image transfer end to end.
Stock infection control supplies.
Document a backup route plan.
What this hides is throughput risk. Year 1 assumes 3 X-ray techs at 300 monthly studies per tech and 2 ultrasound techs at 180 monthly studies per tech. If equipment readiness is weak, that capacity never turns into revenue, and opening-day schedules turn into canceled visits.
2
Clinical Staffing And Radiologist Workflow
Clinical Staffing and Report Flow
This driver decides whether you can open on time and serve patients on day one. The readiness signal is credentialed technologists scheduled, lead technologist oversight defined, radiologist or teleradiology coverage contracted, and report turnaround standards written. If those pieces are late, you can still market the service, but you can’t deliver clean studies or reliable reports.
The Year 1 staffing plan of 3 X-ray techs, 2 ultrasound techs, 1 lead technologist, 1 patient coordinator, and 1 client relations role only works if hiring, credential checks, patient-handling protocols, quality control, image documentation, and escalation rules are already set. One clean rule: do not book studies until the interpretation workflow is tested.
Lock the workflow before booking
Verify staffing against expected order volume, then schedule coverage around the exams you can actually clear. If the team is thin, route capacity falls fast and turnaround gets messy. That hits compliance, patient experience, and first-revenue timing all at once.
Confirm licenses and credential checks.
Test image transfer and report routing.
Assign one owner for QC escalation.
Write who handles bedside patient flow, who reviews image quality, and who calls for repeats. Also define the lead technologist’s oversight role before launch, because that is what keeps capacity and report timing from breaking in the first busy week.
3
Referral Network And Facility Onboarding
Facility Referral Onboarding
This launch driver matters because mobile imaging volume starts with signed referral accounts, not general awareness. If skilled nursing facilities, assisted living communities, home health agencies, physician groups, urgent care sites, and occupational health accounts are not onboarded before opening, you can have staff and equipment ready but still miss day-one revenue.
The real gate is operational confidence. Facilities need a clear physician order process, service-level expectations, coverage area, and pricing or billing terms before they send the first scheduled orders. Verbal interest is not launch demand, and that gap can delay opening even when the rest of the business is ready.
Turn Interest Into Signed Accounts
Before opening, document the full referral path: who places the order, how it gets approved, how reports return, and who follows up on exceptions. Pair each target facility with an administrator outreach plan, a workflow demo, and an onboarding call so the team can test the process before go-live. One clean handoff matters more than a long prospect list.
Get signed referral terms in writing.
Set order forms before launch.
Confirm coverage area and billing rules.
Test report delivery with one facility.
Assign one owner per account.
If the facility cannot place a real order and get a reliable report back, the launch is not ready. That is the bottleneck that turns a busy sales pipeline into a slow first month.
4
Scheduling, Routing, And Billing Systems
Dispatch and Claims Readiness
Dispatch and claims readiness decides whether mobile imaging can open on time. If orders, routes, appointment windows, image transfer, reports, payer setup, HIPAA communications, and denials tracking are not working together, the first week turns into missed visits and slow cash. One clean claim path matters more than a big launch list.
This driver depends on service area design and payer readiness. Scattered orders can burn fuel and staff hours, and the Year 1 direct procedure assumptions already include 4% consumables and 3% vehicle fuel, so weak routing quickly squeezes margin and adds payment delays.
Test the full intake-to-claim flow
Before opening, test the full chain: referral intake, dispatch rules, route density targets, billing codes, claim workflows, collection follow-up, and secure patient communication. The readiness check should end with a scheduled route, a completed study, a delivered report, and a claim that can move without manual fixes.
Set intake and order fields first.
Map routes by facility density.
Check payer setup before launch.
Track denials from day one.
Use backup plans for late orders.
If the first orders are spread across too wide an area, the team will waste drive time and miss windows. Tight routing and clean billing keep day-one service steady and protect cash while claims move through the system.
5
Financial Runway And Utilization Ramp
Runway Before Ramp
This launch driver matters because mobile imaging can open on time only if cash lasts while volume climbs. The key test is a model that ties daily studies, payer mix, collections timing, technologist hours, vehicle capacity, fixed expenses, and runway together so you can see when the business turns cash-positive, not just revenue-positive.
Here’s the quick math: X-ray at 3 techs, 300 monthly studies per tech, $220 price, and 65% capacity equals about $128,700 a month. Ultrasound at 2 techs, 180 studies per tech, $380 price, and 60% capacity equals about $82,080 a month. Direct procedure costs run 7% total, split between 4% consumables and 3% fuel.
Verify Demand Before Hiring
Before opening, lock the plan to signed referral demand, not hopeful volume. Build the ramp around actual order flow, then match tech hours and vehicle capacity to that pace. If you hire ahead of demand, payroll starts immediately, but collections may lag, which burns runway fast and can force launch delays or a narrower service area.