How To Open A Mobile Mammography Business With 5 Year 1 Techs
You’re launching a regulated breast screening service, so the first job is readiness, not promotion This guide covers the practical mobile mammography launch steps across compliance, vehicle setup, staffing, payer setup, partner sites, scheduling, and first revenue, using a five-year planning period and a Year 1 operating plan with 5 tech roles Validate the route plan before committing to launch
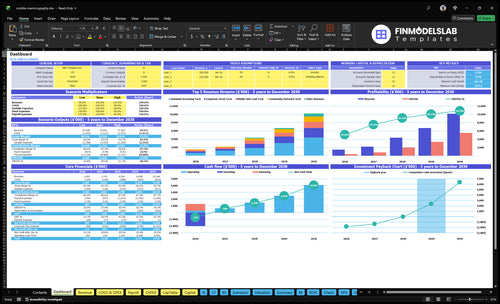
Time to Open6 monthsOpening prepLaunch Sequence6 stagesCompliance firstKey BottleneckCredentialing gapPayer timingFirst Revenue StepBooked eventClaims ready
Launch timeline
This short web summary shows the launch workstreams, and the XLSX export carries the detailed Gantt chart.
How do you get first customers for mobile mammography?
First customers for Mobile Mammography come from booked screening days, not broad awareness: target employers, health systems, obstetrics and gynecology practices, Federally Qualified Health Centers, community groups, insurers, churches, and breast cancer awareness events. For the launch-cost side, see How Much Does It Cost To Open, Start, Launch Your Mobile Mammography Business? because the first revenue path only works when host-site agreements, appointment slots, eligibility checks, payer setup, reminders, image transfer, radiologist reads, claims, and follow-up are in place. Here’s the quick math: 200 corporate screenings at 70% use and $220 each is about $30,800 a month; 150 screenings at 50% and $180 is about $13,500.
First buyers
Employers fill routes fast.
Health systems can refer patients.
FQHCs serve underserved areas.
Churches and events drive bookings.
Must-have setup
Host-site agreement before any visit.
Eligibility and payer checks up front.
Repeat routes cut idle vehicle time.
No-shows and claims timing delay cash.
How long does it take to open a mobile mammography business?
Mobile Mammography usually takes several months to open, because compliance, vehicle buildout, equipment delivery, staffing, and payer credentialing all move on different timelines. Use first week, opening month, and early ramp-up as your model periods, not exact dates; in Year 1, plan for 5 tech roles, 50% to 70% utilization by service line, and 0 premium tech capacity in Years 1 and 2.
What slows launch
Vehicle buildout can add weeks
Imaging equipment delivery can slip
Certification inspections can delay go-live
Technologist hiring can take time
What to do first
Compliance planning starts first
Payer credentialing starts early
IT workflow happens before dry runs
Partner-site scheduling happens before soft launch
What mobile mammography launch mistakes create the most risk?
Mobile Mammography gets risky when you buy equipment before the compliance path is clear, then launch without payer setup, radiologist coverage, or enough host sites. The fastest way to protect safety and cash is a pre-open check on MQSA/FDA readiness, state rules, QA files, HIPAA workflow, billing, partner pipeline, and route calendar. Here’s the quick math: planned utilization should be checked against 60% standard, 50% outreach, 70% corporate, and 65% lead tech, because variable costs are only 14% of revenue, so low route fill hurts fast.
Pre-open checks
Confirm MQSA/FDA readiness
Check state rules first
Complete QA files
Test equipment acceptance
Set HIPAA workflow
Lock billing setup
Build partner pipeline
Map route calendar
Big launch risks
Buy gear too early
Miss payer credentialing time
Launch without radiologists
Book too few sites
Skip recall follow-up
Run low-use routes
Do a full dry run
Test abnormal-result handoff
Key Takeaways
MQSA readiness gates the launch.
Vehicle and equipment setup drives capacity.
Staffing and radiologist coverage set throughput.
Payer setup and partners turn screenings into revenue.
Regulatory And MQSA Readiness
MQSA Readiness
If the mobile unit is not ready for MQSA and state radiology review, it cannot open cleanly on day one. This driver covers the certification path, accreditation plan, medical oversight, QA program, inspection files, and staff credential checks, so it is the gate before patient launch.
Here’s the quick math: the model includes $800 per month for accreditation and licensing fees. That spend is small next to the cost of a delayed opening, because weak compliance usually means retrofitting the operating model after purchase, which drives inspection risk and opening delays.
Lock the compliance path before purchase
Confirm the exact state requirements first, then line up the vehicle, equipment plan, radiologist coverage, and patient record workflow to match them. If those pieces do not fit the MQSA rules, you will waste time fixing a unit that is already built.
Verify state radiology requirements
Document accreditation and licensing steps
Create quality control logs early
Train staff on inspection files
Check every credential before launch
What this avoids is simple: no compliant pathway, no proper patient launch. Strong prep lowers inspection risk and cuts the chance of last-minute delays that stall first-day screenings.
1
Vehicle And Imaging Equipment Setup
Vehicle and Imaging Setup
This is the physical gate to day-one screening. If the van, mammography unit, power, and image transfer are not ready, you can’t open on time, even if the calendar is full. The launch signal is an accepted vehicle buildout with working imaging equipment, tested connectivity, and a flow that protects patient privacy and safety.
Vendor timing is the main risk. One delayed install, weak power setup, or unit that can’t support a compliant workflow can turn booked screening days into cancellations and idle route time. A documented maintenance plan matters too, because the first week of operations needs uptime, not surprises.
Lock the buildout before you sell dates
Start with vendor selection, delivery tracking, and install dates tied to your certification path, IT, insurance, route plan, and partner sites. Then test image transfer, parking access, patient privacy, and safe patient flow before the first booking. That tells you if the unit can actually screen, not just sit in a lot.
One clean rule: if the van can’t move images and patients safely, it’s not launch-ready. Keep contingency plans for a backup site, a delayed install, and maintenance hold time so a single equipment miss does not break the week.
Confirm coach and equipment delivery dates.
Test power and connectivity twice.
Document maintenance and QA checks.
Verify parking and host-site access.
2
Clinical Staffing And Radiologist Coverage
Clinical Staffing and Radiologist Coverage
Day-one capacity in mobile mammography is only as good as the technologists and radiologist behind it. The Year 1 plan calls for 2 standard screening techs, 1 community outreach tech, 1 corporate event tech, and 1 mobile unit lead tech, plus an interpreting radiologist and supervising physician structure. Without those roles, you can book visits but you cannot safely screen, read, and close the loop.
The real risk is speed mismatch: if you screen patients faster than images can be read, follow-up stalls and the patient experience breaks. That also affects MQSA readiness, payer credentialing, route timing, and recall workflow, so weak coverage can delay opening even when the vehicle is ready.
Lock Coverage Before Booking
Before launch, verify every technologist credential, lock the radiologist contract, and assign backup coverage for absences. Build written turnaround standards for image reads, patient scripts for normal and abnormal results, and an escalation path for delayed reads. The Year 1 model includes 5% radiologist reading fees, so coverage has to match the screening schedule.
Here’s the quick sequence: staff schedules first, route calendar second, intake support third, and recall workflow last. If any link slips, the clinic can still open, but same-day throughput falls and handoffs get messy.
Check technologist licenses and certification
Confirm radiologist read-time targets
Define backup coverage for absences
Test intake and patient communication scripts
Assign recall and escalation ownership
Match staffing to route calendar volume
3
Payer Credentialing And Billing Readiness
Billing Ready Before Day One
Payer credentialing is what turns each screening into collectible revenue. For a mobile mammography launch, that means commercial insurance setup, Medicare and Medicaid considerations, coding rules, eligibility checks, claims submission, and denial handling. If this runs late, you can still screen patients, but day-one cash slips and write-offs rise.
Here’s the quick math: Year 1 prices are $250 standard, $180 outreach, $220 corporate, and $250 lead tech screening. Those rates only matter if the legal entity, provider setup, radiologist arrangements, and intake data are ready for clean claims. One missing payer step can block billing on the first event.
Verify Claims Flow Before Booking
Start credentialing applications early and track each payer contract in one file. Run a claim test process, review coding, verify benefits, and assign one owner to the denial queue. That keeps the first screenings tied to a real collection path, not just booked volume.
The main risk is booking events before claims can be filed correctly. So, confirm patient billing rules, scheduling system fields, and intake data before opening the calendar. If those pieces are weak, the team spends opening week fixing claims instead of serving patients.
Confirm payer enrollment status.
Test claims before first event.
Assign denial queue ownership.
Verify Medicare and Medicaid rules.
Match intake data to billing.
4
Partner Site Pipeline
Partner Site Pipeline
This driver decides whether the unit opens with booked screening days or sits compliant but idle. For a mobile mammography business, the pipeline means signed or confirmed sites, appointment targets, host-site logistics, referral partners, repeat route potential, and the right patient mix before the vehicle rolls.
The real risk is a compliant unit with too few booked screening days. If employer outreach, clinic referral agreements, community health ties, and pre-registration are not done early, day-one operations can start late or with weak volume, which hits first revenue and wastes staffed time.
Prebook the route, not just the van
Lock the site list before launch: employers, clinics, churches, community events, and insurer-linked channels. Check parking, power, patient flow, and follow-up workflow at each site, then match those sites to payer-fit patient mix and screening-day targets.
Here’s the quick math: at 200 monthly screenings per tech and a $220 price, one fully used tech can support about $44,000 in monthly gross volume. Year 1 utilization is modeled at 70%, so every weak site or empty day cuts early cash and leaves fixed staffing and vehicle costs spread over fewer visits.
Confirm site dates in writing.
Verify parking and patient access.
Pre-register patients before arrival.
Track repeat route potential.
Match sites to payer mix.
5
Scheduling, Routing, And Follow-Up Operations
Scheduling And Follow-Up Control
For mobile mammography, scheduling is what turns booked demand into completed, billable visits. The launch only works if appointment booking, eligibility checks, route planning, reminders, intake forms, image transfer, results communication, recall management, and abnormal finding follow-up all run cleanly on day one. If any step breaks, you can still have a full calendar and still miss revenue or patient care.
The operating benchmark matters. Year 1 utilization is set at 60% for standard days, 50% for outreach, 70% for corporate, and 65% for the lead tech. That means the schedule has to absorb travel time, no-shows, and follow-up work without pushing the van off route or leaving patients stuck waiting for results.
Build The Booking And Recall Flow First
Before opening, lock the whole chain: build scheduling templates, set route density targets, test reminders, confirm host-site arrival workflow, connect PACS/RIS and EHR interfaces, and assign one owner for abnormal results and recalls. PACS/RIS is the imaging and radiology record flow, and EHR is the electronic health record. If those links are late, day-one volume can look real but fail in follow-up.
Set route density before booking dates.
Test reminder texts and calls.
Confirm patient intake and arrival steps.
Assign results and recall ownership.
Verify HIPAA workflows before launch.
The key dependencies are payer setup, radiologist coverage, partner sites, vehicle reliability, and HIPAA workflow. If any one slips, you risk lost revenue from unbilled visits or patient harm from missed results. That makes follow-up a launch control point, not an admin task.