Start an Outpatient Surgical Center With a 12-24 Month Launch Plan
To open an outpatient surgical center, start with feasibility, specialty mix, state licensing, facility buildout, accreditation or Medicare readiness, staffing, payer contracting, and revenue cycle setup A practical planning range is 12-24 months, but certificate of need rules, construction scope, inspections, credentialing, and payer contracts can stretch that The researched Year 1 staffing plan uses 2 surgeons, 2 anesthesiologists, 4 registered nurses, 4 surgical technicians, and 2 recovery nurses, with capacity assumptions of 60%-65% First revenue should come from scheduled, contracted cases billed through a tested revenue cycle
Time to Open12-24 monthsLaunch runwayLaunch Sequence7 stagesFeasibility firstKey BottleneckLicense gateApproval pathFirst Revenue StepFirst casesBilling live
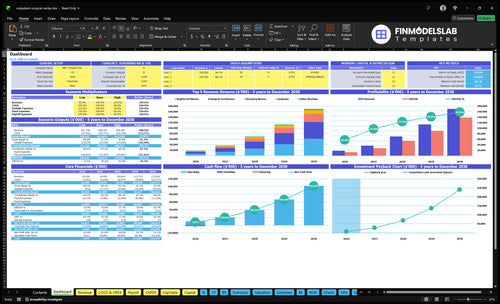
Launch timeline
This is a short web summary of the launch plan; the XLSX export carries the detailed Gantt chart and readiness gates.
How do outpatient surgical centers get patients and first cases?
An Outpatient Surgical Center usually gets its first patients from surgeon partners and recruited physicians who bring eligible same-day cases. For launch planning, the Year 1 model assumes 2 surgeons and 2 anesthesiologists at 20 monthly treatments each, but only about 60%–65% of capacity at first. The first cases only turn into revenue when they’re contracted, authorized, scheduled, coded, and billed cleanly, and What Is The Estimated Cost To Open And Launch Your Outpatient Surgical Center? matters because weak surgeon commitments are the biggest early blocker.
How first cases arrive
Surgeon partners drive early volume
Recruited physicians bring eligible cases
Specialty mix shapes case flow
Block scheduling protects access
What can stall revenue
Weak surgeon commitments delay volume
Uncontracted cases don’t pay
Missing prior authorization slows billing
Clean claim submission keeps cash moving
What licenses are needed to open an outpatient surgical center?
To open an Outpatient Surgical Center, plan for entity formation, a state facility license, zoning/building/fire approvals, infection control standards, and a Medicare certification or accreditation path; start before lease signing because CON, surveys, and inspections can control the timeline. Requirements vary by state, so verify whether a Certificate of Need applies; What Is The Current Growth Trajectory Of Outpatient Surgical Center? matters, but compliance is the gate that lets revenue start.
What outpatient surgical center launch mistakes create the most risk?
The biggest launch risk for an Outpatient Surgical Center is opening before the basics are live: licensing, payer contracts, surgeon privileges, and transfer arrangements. That can stall cash fast, because one bad first claim or a missing anesthesia shift can slow the whole start. Here’s the quick read: run a full readiness check, then test scheduling through claim submission before the first case.
Regulatory and payer risk
Don’t miss licensing timelines.
Check certificate of need rules.
Activate payer contracts first.
Confirm surgeon privileges early.
Operations and cash risk
Lock the first-case calendar.
Test sterile processing workflows.
Verify anesthesia coverage gaps.
Update for delayed Year 1 capacity.
Key Takeaways
Regulatory approval sets the legal launch date.
Facility buildout must match surgery, sterilization, and safety flow.
Two surgeons drive Year 1 ramp and case volume.
Billing, staffing, and payer setup protect early cash.
Regulatory Approval And Accreditation
Regulatory Approval And Accreditation
This is the gatekeeper for opening. An outpatient surgical center can’t legally open and bill eligible cases until the state facility license is in hand, and some states also require a certificate of need. Fire and life safety approvals, infection control documents, survey evidence, and emergency transfer plans all have to line up before first cases.
The risk is simple: if you wait until late buildout to confirm state rules, you can trigger rework, delay inspections, and push back your first-case date. This driver depends on the site, buildout, equipment, staffing files, and clinical policies being ready at the same time.
Confirm the rule set early
Before spending hard on finish-outs, verify the exact state licensing path and whether accreditation or Medicare certification is needed. Build the file set around what surveyors will ask for: policies, infection control, emergency transfer agreements, and proof the facility matches the approved use.
Lock the license path first.
Match policies to survey rules.
Document transfer coverage now.
Stage evidence before inspection.
That sequencing cuts inspection rework and makes first-case timing clearer. If one approval slips, the opening date can move even when the rooms are built and the staff is hired.
1
Facility Buildout And Equipment
Facility Buildout And Equipment
This driver decides whether the outpatient surgical center can safely run same-day surgery on day one. The layout has to connect the operating room, pre-op, recovery, sterile processing, anesthesia space, supply storage, infection control flow, and emergency systems. If one piece is missing, you can still have staff on site but no usable surgery day, which pushes opening back and raises first-case cancellation risk.
The buildout also has to match the specialty mix and equipment list. Different procedures need different instruments, anesthesia support, and clean-to-dirty flow. If vendor timing slips or the room setup misses survey standards, you get rework, delayed inspections, and a weaker start. Here’s the quick math: no ready room means no billable case, even if the schedule is full.
Precheck the room flow before ordering gear
Lock the room map first, then buy equipment against that map. Confirm the operating room, pre-op, recovery, sterile processing, and storage areas fit the planned cases, and verify the clean/dirty path, anesthesia setup, and emergency response gear before final inspection. That keeps the buildout tied to actual day-one use, not just a floor plan.
Test the flow with a mock first case, then fix gaps in sterilization, emergency backup, or anesthesia access before opening. Document vendor dates, room-by-room responsibilities, and inspection items so nothing gets left to the last week. If those details slip, inspectors see rework and the first cases are the ones most likely to get cancelled.
2
Surgeon Case Pipeline
Surgeon Case Pipeline
This driver decides whether an outpatient surgical center has real cases on day one or just an open building. You need committed surgeons, approved privileges, a defined same-day case list, and block schedules before opening, or the OR sits idle while payroll and rent start. Verbal interest is not enough; scheduled, contracted cases are what turn readiness into first revenue.
Here’s the quick math: the Year 1 model assumes 2 surgeons, 20 monthly treatments per surgeon category, and a $5,500 treatment price, or 40 treatments and about $220,000 a month at full plan. If launch starts at 60% capacity, that is closer to 24 treatments and $132,000 monthly, so early ramp depends on how fast surgeon blocks and referrals are actually locked in.
Lock Cases Before Opening
Sequence the pipeline before the opening date: confirm surgeon commitments, match each specialty to facility capability, approve privileges, and load block time into the schedule. Keep the case list tight to same-day procedures that fit the center’s equipment, staff, and anesthesia plan, so you do not promise surgeries you cannot safely support.
Use a simple launch check: signed surgeon intent, approved privileges, defined procedure mix, and referral flow all in place before first case day. If any of those are missing, opening may still happen, but the center will likely start with weak utilization, more cancellations, and slower cash collection.
Get signed block commitments early.
Match cases to facility limits.
Confirm referral sources before launch.
Track capacity at 60% start.
3
Payer Contracting And Credentialing
Payer Contracting And Credentialing
Payer contracting and credentialing decide whether first cases become collectible revenue. The center needs payer enrollment, managed care contracts, reimbursement schedules, prior authorization rules, eligibility checks, patient financial clearance, and billing-system contract loading before opening. The key dependency is a clean legal entity, active licenses, provider files, specialty mix, and a real case pipeline.
If the center plans for 2 surgeons, 20 monthly treatments per surgeon category, and $5,500 per treatment, a late payer setup can stall meaningful cash in month one. Open before contracts and authorizations are live, and you get denials, slower collections, and a weaker cash runway. One clean rule: no active payer path, no day-one schedule.
Launch Readiness Checks
Start payer work before the schedule hardens. Credentialing and enrollment often run 30-90 days when provider files or contract data are messy, so verify every payer file, then test prior auth and eligibility in the billing system before the first case date. That keeps the first claims clean instead of pushing fixes into collections.
Confirm legal entity and licenses.
Match specialties to payer rules.
Load contracts into billing.
Test prior auth and eligibility.
Clear patient balances before surgery.
4
Clinical Staffing And Anesthesia Coverage
Day-One Clinical Coverage
Clinical staffing and anesthesia coverage decides whether the ASC can open with safe first cases. You need credentialed surgeons, anesthesiologists, registered nurses, surgical technicians, recovery nurses, sterile processing support, and administrator oversight. If any file is late, the center may have to delay cases or run short on coverage, which hurts on-time opening and day-one throughput.
The Year 1 plan calls for 2 surgeons, 2 anesthesiologists, 4 registered nurses, 4 surgical technicians, and 2 recovery nurses. That staffing mix only works if competencies, call coverage, and schedule templates are built before opening. One missing clinician can force case changes, stagger starts, or cancel the first surgical day.
Pre-Open Staffing Check
Start credentialing early and track each file to a hard go-live date. The launch risk is simple: hiring too late or waiting on approvals creates empty rooms and canceled cases. Here’s the quick check: confirm every clinician is cleared, trained, and slotted into the template before the first patient arrives.
Verify credentials before scheduling.
Lock call coverage for case days.
Test competencies on center workflows.
Match templates to planned volume.
What this hides: if one role slips, the whole day can slip. Safer first cases come from staffing that is signed, trained, and ready to work on day one.
5
Revenue Cycle And Operating Workflows
Cash-Ready Revenue Cycle
For an outpatient surgical center, this driver decides whether first cases turn into cash on time or sit in billing limbo. The work includes scheduling, eligibility checks, prior authorization, coding, charge capture, claims submission, and denial tracking, plus implant and supply controls and EHR setup.
The risk is simple: if you treat patients before claims, charges, and supply workflows are tested, you can open the doors but still miss revenue. With Year 1 variable expense assumptions of 40% billing and collections fees, 10% EHR transaction fees, 90% medical and surgical supplies, and 15% sterilization supplies, cash conversion needs to work from day one. Cleaner billing means fewer surprises.
Test Before First Case
Build the full case flow before opening: schedule the patient, verify eligibility, obtain prior auth, confirm the code set, capture charges the same day, submit the claim, and log every denial. Also check sterilization logs, implant traceability, and vendor fill rates so missing supplies do not cancel a case after the patient is prepped.
Here’s the quick rule: no live cases until EHR workflows, billing rules, and supply controls work on paper and in a test run. Assign one owner for claims, one for supplies, and one for vendor follow-up. If any step breaks, cash slows, rework rises, and day-one operations get noisy fast.