How To Start A Medical Prior Authorization Service In 6 To 12 Weeks
A lean medical prior authorization service can often launch in about 6 to 12 weeks if compliance documents, Business Associate Agreements, secure systems, payer portal access, EHR permissions, staff training, pricing, and provider outreach are ready The researched planning model assumes Month 1 setup, breakeven in Month 7, minimum cash of $519,000 in Month 6, and first-year revenue of $1287 million The main bottleneck is not the website it’s getting provider trust, EHR access, payer credentials, and payer-specific workflows live First revenue starts when a provider agreement is signed and completed authorizations are billed under the agreed fee model
Time to Open6-12 weeksLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckPortal accessProvider trustFirst Revenue StepSigned clientAuths billed
Launch timeline
This is the short web summary of the launch plan, and the XLSX export contains the detailed Gantt Chart.
What mistakes create the biggest prior authorization service risks?
For a Medical Prior Authorization Service, the biggest risk is launching without payer-specific SOPs and clear documentation rules; that usually drives denials, slow turnaround, and weaker provider trust. A pre-launch risk check should cover HIPAA controls, escalation, quality review, status reporting, and cash runway. If volume grows faster than 3 Year 1 authorization specialists can handle, provider satisfaction drops.
Top launch risks
No payer-specific SOPs
Unclear clinical rules
Weak HIPAA controls
No urgent-request staffing plan
What slips go-live
No escalation process
No quality review
No status reporting
Late EHR access or undertrained staff
How do you get clients for a prior authorization service?
Start with a tight niche that already feels authorization pain, like high-volume specialties, and sell faster turnaround, cleaner documentation, live status visibility, and fewer missed follow-ups. If you’re pricing the work, What Are Operating Costs For Medical Prior Authorization Service? helps frame the cost stack. With a $120,000 year-1 marketing budget and $2,400 customer acquisition cost (CAC), the plan models about 50 accounts if spend converts as expected.
Best-fit clients
Target high-volume specialties first
Lead with faster turnaround
Show cleaner documentation
Promise fewer missed follow-ups
First-sale offer
Use a signed provider agreement
Include a BAA
Add an onboarding checklist
Attach a reporting sample and fee model
First revenue comes from completed authorizations and implementation service billing, so the pilot should be simple to buy and easy to start.
How long does it take to start a prior authorization service?
For Medical Prior Authorization Service, a lean launch usually takes 6 to 12 weeks, because the real delay is provider-side coordination, not basic business registration. The work has to run in order: compliance first, then systems, then access, then SOPs, then a pilot provider. In the model, Month 1 is setup, Month 6 is the minimum cash need, and Month 7 is breakeven.
Why it slows down
Provider agreements take time
Payer portal credentials must clear
EHR permissions need setup
HIPAA documents come first
Launch sequence
Start with compliance work
Set up systems next
Then secure access and workflows
Train staff before the pilot
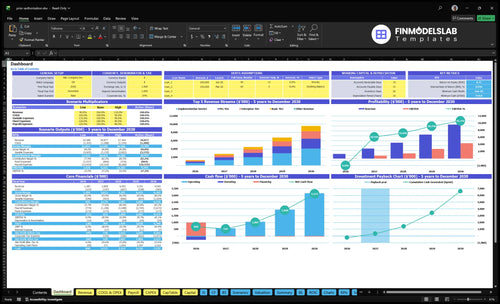
Medical Prior Authorization Service Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Validate whether the prior authorization service is ready to open
Launch readiness checklist
Use this go-live approval checklist before opening the medical prior authorization service.
1Compliance
BAAs signed with vendorsCritical
No BAA means no launch with protected health information (PHI).
HIPAA policies approved and publishedCritical
Staff need one rule set for privacy, access, and incidents.
Liability insurance bound before go-liveHigh
Coverage should start before patient data work and provider contracts.
Access controls limit record exposureCritical
Least-privilege access keeps record exposure tight.
Audit logs reviewed for traceabilityHigh
Audit logs prove who touched each request.
2Payer setup
Provider contracts signed for launchCritical
Signed contracts set scope, fees, and launch coverage.
Payer portal access testedCritical
If portal access fails, requests stall and revenue slips.
EHR user roles approvedHigh
EHR (electronic health record) roles keep staff out of the wrong records.
Documentation rules confirmedHigh
Clear intake rules stop rework when payers ask for more.
3Platform
Secure hosting meets HIPAA controlsCritical
Hosting must protect data, access, and backups.
Integration workflow passes end-to-endCritical
Test the full path so submissions do not break.
Backups restore cleanly in testHigh
A failed restore can stop service after an outage.
Audit trails capture every actionHigh
Audit logs help resolve payer disputes fast.
4Operations
Specialty SOPs signed offCritical
Specialty-specific steps cut denials and rework.
Service-level targets agreedHigh
Set response times and update cadence now.
Escalation rules documented and sharedCritical
Staff need a clear path when blockers hit.
Denial tracking dashboard readyHigh
Track denials early and fix root causes.
Reporting cadence set with clientsMedium
Providers need steady updates to trust the process.
Year 1 starts with these core roles plus three auth specialists.
Three auth specialists onboardedCritical
Month 1 capacity starts here, so hires must be ready before launch.
Workflow training completedHigh
Training must cover payer steps, EHR use, and denial handling.
Launch coverage schedule approvedHigh
Coverage must match expected request volume on day one.
6Revenue
Pricing tiers approved for launchHigh
Use the approved tiers so revenue lines up with the model.
Signed provider ready for intakeCritical
A signed provider plus live workflow is the first revenue proof.
Month 1 overhead fully fundedCritical
Fixed overhead is $14,400 before wages, so cash must cover more than payroll.
Cash runway reaches Month 6Critical
Minimum cash lands in Month 6, so funding must bridge the first six months.
Owner signs go-live approvalCritical
This final signoff should follow tested access, trained staff, and signed contracts.
Which launch drivers matter most before go-live?
1Compliance & BAAs
BAAs signed
Signed BAAs and HIPAA controls speed trust and keep the 6-12 week launch path on track.
2Payer Access
Go-live access
Permissioned payer and EHR access turns trained staff into live submission capacity.
3Specialty SOPs
SOP tested
Specialty SOPs reduce rework and denials, so turnaround stays tighter.
4Trained Staff
3 specialists
Three specialists set day-one capacity and keep urgent requests moving.
5Provider Sales
$1.287M
Pilot accounts at $1,200 to $5,000 monthly create first revenue and validate demand.
6Reporting Capacity
$519K
A live queue dashboard spots backlog early and protects the $519K cash floor in Month 6.
Compliance And BAAs
HIPAA And BAAs
No signed BAA, no live work. A prior authorization service touches protected health information, so day one readiness depends on HIPAA policies, secure hosting, access controls, audit logs, staff training, and insurance being in place before the first request goes out.
The main bottleneck is provider legal review. If the contract sits with counsel or privacy terms feel weak, onboarding stalls before launch. A complete compliance packet speeds trust, cuts back-and-forth, and keeps the team from opening with a process they can’t legally run.
Lock the privacy package early
Build the compliance set before sales closes the first account. Here’s the quick order: policies, BAA template, hosting review, user permissions, audit logging, staff training, and insurance proof. The goal is simple: a provider can sign once and start without a second legal pass.
Set 0 live requests without BAA
Confirm 100% staff training before go-live
Assign one legal owner
Test access before live work
Keep insurance certificates current
What this hides: one missing control can slow launch more than the software build. A clean package reduces privacy concern, shortens contract delay, and prevents a day-one problem where staff are ready but blocked from touching protected health information.
1
Payer Portal And EHR Access
Payer And EHR Access
This driver sets the real go-live date. Prior authorization work only starts when the team has permissioned user access, payer credential steps done, and provider-approved workflows loaded into the EHR. If those accounts are not live, staff can be trained and still be unable to submit, track, or update requests, which means no day one operating capacity.
It also covers test submissions, role limits, multi-factor access, payer-specific portal mapping, and status update rules. The launch fails if the team cannot see case status or send clean requests through the right portal. That creates idle payroll, delayed first revenue, and avoidable provider frustration because the service exists on paper but not in practice.
Lock Access Before You Schedule Go-Live
Verify every payer login, EHR permission, and approval path before the open date. Assign one owner to track user provisioning, role limits, and multi-factor setup, then map each payer to the right portal and status workflow. One blocked account can stop the whole launch if that payer is part of the first client mix.
Run test cases with real request types, then confirm the team can submit, save notes, and pull status updates without provider help. Document who can enter, who can edit, and who can close a request. If the workflow is not live in the system, the service is not ready to bill or scale.
Confirm payer credentials first.
Test submission and status tracking.
Set role-based access limits.
Match workflows to each payer.
2
Specialty Workflow SOPs
Specialty Workflow SOPs
A generic prior authorization SOP can slow launch on day one. Specialty clinics need a workflow that matches specialty needs, payer rules, and the right CPT and HCPCS codes, plus the medical necessity documentation and clinical attachments each payer expects, or first submissions will bounce back.
The readiness signal is a tested checklist for each service line and payer pattern, with clear status checks and escalation steps. Without that, the team burns time on rework and avoidable denials, and turnaround slips right when the clinic expects live support.
Test the payer checklist first
Before opening, map each specialty to the exact documents, codes, and follow-up steps. Include denial reason logging, missing-document follow-up, an urgent-request path, and quality review so the team can fix gaps before they hit the payer.
Run the checklist on real request types, then confirm who owns updates, who escalates, and when. If one payer pattern is still manual, you can still open, but first-week capacity will be tight and avoidable back-and-forth will slow early revenue.
3
Trained Authorization Staff
Trained Authorization Staff
Day-one capacity depends on people, not just software. For a medical prior authorization service, trained specialists set the pace for submissions, payer follow-up, and appeal work. The Year 1 staffing plan assumes 3 authorization specialists at $65,000 each, or about $195,000 per year before taxes and benefits. If you start with fewer staff, turnaround time slips fast and provider trust drops.
Readiness means staff can handle payer experience, specialty rules, QA review, urgent requests, and clear escalation paths. If a complex case lands with someone untrained, you risk rework, missed status checks, and slower approvals on opening week. That can block first revenue because providers expect the service to work from day one. Untrained hands create backlogs fast.
Hire and Train Before the Queue Opens
Build the team before live work starts. Use training scripts, shadow review, escalation rules, and backlog monitoring so every specialist knows when to act, when to ask, and when to hand off. Set defined productivity targets up front so you can see whether staffing matches demand, not guess after the queue is already behind.
Train on payer-specific work first.
Shadow every new specialist.
Test urgent-request coverage.
Track backlog daily.
The main launch risk is hiring too late or loading complex requests onto new staff too soon. That delays turnaround, raises provider frustration, and can push opening past the point where the service looks reliable. Start with enough coverage to handle normal flow plus urgent cases, then watch volume against the 3-person staffing plan.
4
Provider Acquisition And Pricing
Provider Niche and Pricing
A prior authorization service can’t open commercially without a clear provider niche, a signed agreement, an onboarding path, and a first pilot account. The Year 1 mix of 45% Basic at $1,200, 40% Pro at $2,500, and 15% Enterprise at $5,000 implies a weighted recurring price of $2,290 per active client, plus a $2,000 implementation fee.
Broad outreach without proof is the launch risk. It can create interest, but not signed pilots, and that pushes back first revenue and hides true capacity. One clean line: no niche, no fast launch.
Price the Pilot First
Before opening, lock the niche, package, and handoff in writing. Confirm what the provider signs, what data is needed to start, who owns onboarding, and when implementation is billed. The first account should test the full path from signature to live work, not just a demo.
Set one niche and one pilot
Match price to workload
Document setup steps and owners
Bill implementation at kickoff
Track time to first authorization
Use the pilot to test capacity math. If one client takes longer than planned to onboard, staffing needs and cash timing will be off. Track setup time, open tasks, and the date of first authorization so you know if the model can support day-one operations.
5
Reporting And Capacity Management
Reporting and capacity control
Prior authorization reporting is a day-one control, not a nice-to-have. If the dashboard is not live at opening, the founder cannot see turnaround time, open requests, payer aging, missing documents, denial reasons, completed authorizations, or staff load, so backlog can grow invisibly and service levels slip before the first renewal cycle.
That matters because the service sells speed and proof. Provider-facing reports should show what is stuck, what is done, and where payers are slowing work, or the team may look busy while cash and patient care are delayed. With a planned 3-specialist staffing model at $65,000 each, reporting is what tells you when volume is too high and hiring must start.
Build the queue dashboard first
Set up the dashboard before launch and test it with a few real cases. The minimum inputs are request date, payer, service line, missing documents, denial reason, status, owner, and next action. Without those fields, the team can’t spot bottlenecks or give providers a clean update.
Review the queue daily.
Flag aged requests by payer.
Trigger help when backlog rises.
Send provider reports on schedule.
Track completed authorizations and denials.
Use capacity triggers tied to workload, not guesswork. If open requests climb faster than completed authorizations, or one staffer carries most of the aging cases, that is your launch warning. Fix the report flow first, then scale the team and renewals.
Yes, it can operate remotely if secure systems, HIPAA policies, Business Associate Agreements, access controls, and staff training are in place The model includes HIPAA cloud hosting and data security at 8 percent of Year 1 revenue, plus software and CRM at $1,800 per month Remote work still needs payer portal permissions, EHR access rules, and audit-ready workflows
Start with providers that face steady authorization volume and clear documentation patterns The practical screen is not specialty prestige it’s repeatable requests, payer complexity, and willingness to outsource The Year 1 model assumes Basic, Pro, and Enterprise tiers at 45 percent, 40 percent, and 15 percent of customers, so niche choice should match service depth
You need secure communication, CRM, task tracking, reporting, payer portal procedures, and EHR access workflows The plan includes $1,800 per month for software subscriptions and CRM, plus a $120,000 EHR integration software build over the first six months Keep the first stack simple enough for staff to use daily
Yes, medical billing or revenue cycle experience helps because prior authorization work sits close to coding, payer rules, documentation, and denials It does not replace HIPAA training, payer-specific SOPs, or provider onboarding The model also includes referral commissions to revenue cycle partners at 10 percent of Year 1 revenue, which can support early client acquisition
Hire before go-live only when provider demand, payer access, and training materials are ready The Year 1 plan starts with 3 authorization specialists, then scales to 6 in Year 2 and 12 in Year 3 If you hire too early, cash burn rises if you hire too late, turnaround time and provider trust suffer
About the author
Samuel Price
Launch Planning Specialist
Samuel Price is a launch planning specialist at Financial Models Lab who helps side-hustle builders test whether a business idea is financially realistic. He turns business questions into clear planning steps, with a focus on operating cost estimates for opening and running small businesses. His research-based writing highlights the common costs new founders often miss.
Choosing a selection results in a full page refresh.