How to Open a Psychology Private Practice in 8–20 Weeks
To open a psychologist practice, confirm active state licensure, register the business, secure malpractice coverage, set up HIPAA-compliant systems, choose private pay or payer credentialing, and build referral channels before taking clients A private-pay launch can move faster, while an insurance-based launch often pushes the timeline toward 8 to 20 weeks because credentialing and contracts drive the schedule The researched planning assumptions show Year 1 modeled monthly revenue of about $515k at stated capacity, with payment, EHR, marketing, and referral costs totaling about 13% of revenue The main bottleneck is not the office opening it’s getting reimbursable clients, clean intake workflows, and enough booked sessions to cover fixed overhead
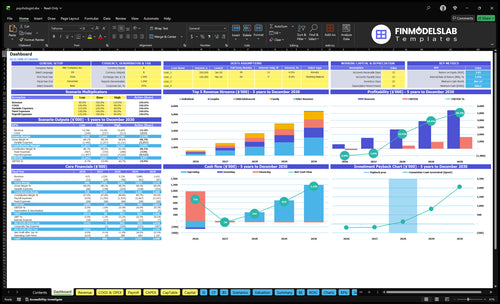
Time to Open8-20 weeksSetup windowLaunch Sequence5 stagesLicense firstKey BottleneckCredentialing delayPayer lead timeFirst Revenue StepBooked intakeIntake ready
Launch timeline
This is a short web summary of the launch plan, and the XLSX export contains the task-level Gantt Chart.
How long does insurance credentialing take when opening a private practice?
Insurance credentialing for a Psychologist private practice usually takes 8 to 20 weeks. Private-pay can start sooner, once licensure, malpractice coverage, HIPAA systems, intake, billing, and referral channels are ready. If rent starts in Month 1 at $4,000, delays burn runway, so run private-pay readiness and payer credentialing in parallel.
Private-pay launch
Start after licensure is active
Confirm malpractice coverage first
Set up HIPAA-compliant systems
Have intake and billing ready
Insurance launch
CAQH and payer apps add time
Contract review creates delays
Effective dates can lag weeks
EHR billing setup must align
What mistakes delay a psychology private practice launch?
If credentialing isn’t clear, a Psychologist private practice can’t count on insurance cash, and weak referrals or no intake flow will leave sessions empty. Here’s the quick math: with $4,000 rent and $5,650 in fixed non-wage overhead, you’re already at $9,650 a month before wages, so launch spend has to match booked sessions, not hope. The usual fix is simple: confirm the payer path, map the 8 to 20 week launch steps, test EHR and billing, and set weekly outreach.
Launch mistakes
Credentialing delays insurance revenue
Weak referrals leave capacity unused
No intake process raises drop-off
Documentation cuts billable time
Fix first
Confirm payer path before opening
Map 8 to 20 weeks of tasks
Test EHR and billing early
Track referrals and booked sessions weekly
What are the requirements to open a psychology private practice?
To open a Psychologist private practice, the go/no-go requirement is an active state psychology license; verify scope of practice and supervision rules with your state psychology board before client care. Then register the business, set taxes, secure malpractice coverage modeled at $250/month, and build privacy, records, consent, intake, billing, and client communication systems; track the operating side with What Is The Most Important Indicator For The Success Of Your Psychology Practice?.
Required First
Hold an active state license
Verify state supervision rules
Register entity and taxes
Buy malpractice before care
Launch Order
Set HIPAA privacy systems
Prepare consent and intake forms
Add 10-digit NPI for insurance
Complete CAQH and referral plan
Key Takeaways
No licensure, no client care, no launch.
Payer choice drives cash timing and admin load.
Test systems before opening to avoid billing delays.
Don’t add rent or staff before bookings.
Licensure and Compliance Readiness
Licensure First
No active state license means no client care. For a psychologist private practice, this is the real go or no-go gate. If licensure, scope rules, malpractice coverage, privacy policies, consent forms, and documentation standards are not ready, the opening stalls and first revenue slips.
No license, no sessions. A prior employer’s compliance process does not carry over, so the founder still has to confirm state board rules, business registration, and secure records setup before day one. That is what keeps the launch defensible and avoids early legal or billing delays.
Pre-Open Compliance Check
Here’s the quick sequence: verify the license, check state board rules, bind malpractice coverage, document the HIPAA privacy process, and test client forms before launch. Readiness means every step works without a manual workaround.
Test the full intake path before opening: can a client book, sign consent, complete documentation, and land in secure records cleanly? If not, the practice may look open but still run into delays, weak first-day service, and avoidable compliance risk.
Verify active license status.
Check scope and board rules.
Bind malpractice coverage.
Test consent and intake forms.
Confirm secure records setup.
1
Payer Strategy and Revenue Access
Revenue Access and Payer Mix
Payer strategy can make the difference between opening on time and waiting weeks for first reimbursed revenue. If the practice starts private-pay, it can bill from day one at $175 for individual, $225 for couples, $250 for family, and $180 for child/adolescent sessions.
If the model includes insurance, credentialing becomes a launch gate. Payer approval can stretch the 8 to 20 week timeline, so the launch date depends on whether the fee schedule, payer list, and billing rules are already locked. A hybrid model can work, but only if the cash timing and admin load are planned upfront.
Sequence Payer Setup Before Opening
Map the revenue path before you schedule the first client. Readiness means the fee schedule, payer list, CAQH profile if needed, contracts, billing workflow, and client payment process are clear enough that staff can collect and post payments without guessing.
Confirm private-pay or insurance mix.
Test the client payment process.
Load all session prices correctly.
Track credentialing dates weekly.
Assign billing ownership before launch.
Weak setup here usually shows up fast: delayed claims, messy intake, and slower cash in the first month. That also changes the marketing message, because a private-pay practice sells speed and simplicity, while an insurance-based practice needs tighter admin handling from the start.
2
HIPAA Systems and Clinical Operations
HIPAA-Ready Client Workflow
For a psychology practice, HIPAA systems are a day-one launch gate, not back-office cleanup. You need secure scheduling, intake forms, consent documents, clinical notes, billing, telehealth, a client portal, and crisis-response procedures working together so a client can book, complete paperwork, attend, get documentation, and pay without manual fixes.
The readiness test is simple: a test client can move through the full flow on their own. If tools are disconnected, documentation slows, billing gets messy, and revenue capture slips. Modeled software costs are $300 per month for the EHR, $200 per month for telehealth, plus 0.5% of Year 1 revenue in EHR transaction fees.
Pre-Open Systems Test
Before opening, run one full dry test and time every step. The system should let a client schedule, sign forms, join telehealth, receive notes or documents, and pay with no staff workaround. If any step needs a manual email, copy-paste, or separate tool, the launch is not ready.
Verify secure scheduling is live.
Test intake and consent forms.
Confirm notes are stored safely.
Check billing and payment flow.
Practice crisis-response handoff steps.
Assign one person to own the workflow map, one person to test it, and one person to fix gaps before opening. The goal is clean operations from day one, not a patchwork that slows sessions and delays cash.
3
Referral and Marketing Pipeline
Referral Pipeline Ready
For a psychologist practice, referrals and local visibility often drive the first bookings. If outreach starts after opening, the calendar can sit empty, which delays cash flow and wastes clinical time. Year 1 marketing is modeled at 8% of revenue, with referral costs at 3%, so this channel has to be ready before the first client day.
What this includes: target clients, service lines, response scripts, a referral list, a tracking sheet, and intake capacity. That means physician outreach, psychiatrist contacts, attorney networks, school counselor relationships, professional directories, and local search setup should be live before opening. No outreach, no first bookings.
Pre-Open Outreach Setup
Build the pipeline before the lease starts, not after. Verify who you want to serve, which services you will offer, and how fast you can answer referred leads. If the phone is slow or intake slots are full, referral partners stop sending names and your first month turns into idle capacity.
Lock the referral list and contact names
Test intake scripts and response timing
Set tracking for source, date, and follow-up
Confirm directory and local search profiles
Match booked slots to opening capacity
The launch risk is simple: waiting until opening month to begin outreach. Start contacts early so the practice can open with real lead flow, not just a website and a hope. That keeps first revenue moving and avoids paying fixed costs for empty time.
4
Office or Telehealth Delivery Setup
Delivery Model Fit
When the service model is not set up right, opening slips fast. An in-person office needs private space, clear scheduling rules, local visibility, and a setup that matches how clients will actually book and show up on day one.
The cost gap matters. Modeled office overhead is $4,000 rent plus $500 utilities and $150 supplies, with a $200 telehealth platform still in the stack. That is about $4,850 per month before staffing. Telehealth-first cuts real estate drag, but it still needs privacy, compliant systems, and emergency steps that work in real time.
Match Setup to Demand
Before signing space, confirm the payer path and referral ramp. That is the bottleneck. If credentialing or referrals are still unclear, a lease can lock in fixed costs before bookings exist, and that slows day-one cash flow.
Use a simple readiness check: private room or secure home office, telehealth tool, client messaging, intake and consent forms, and crisis protocol. If you are choosing hybrid, test both paths before launch so a client can schedule, attend, pay, and get follow-up without manual workarounds.
Verify privacy and sound control.
Test booking and intake flow.
Document emergency response steps.
Keep local visibility aligned.
Avoid lease commitments too early.
5
Capacity, Staffing, and Cash Runway
Capacity, staffing, runway
This launch driver is about whether the practice can actually carry the session load it is promising. The modeled Year 1 revenue is about $515k per month, built on 60% individual, 55% couples, 50% family, and 55% child/adolescent capacity. If weekly sessions, documentation time, and admin work are not sized right, the opening looks ready on paper but slips in the first month.
The cash test matters just as much. Variable costs are about 13% of revenue, fixed non-wage overhead is $5,650 per month, and the Clinical Director salary adds $10,000. That puts monthly fixed pressure at about $15,650 before other pay and growth costs. No-show and billing lag can make a full calendar look better than the bank account.
Plan sessions before hiring
Before opening, map each clinician’s weekly session target against documentation blocks, admin follow-up, and no-show assumptions. Here’s the quick math: if capacity is built from ideal hours instead of real hours, the schedule breaks first in intake, notes, or billing. A test run should show one client can book, be seen, documented, and billed without manual patches.
Set weekly session targets by service line.
Reserve time for notes and admin.
Model no-shows and billing lag.
Verify runway before hiring.
Do not hire or lease ahead of booked demand. The bottleneck risk here is fixed cost: a $5,650 overhead base plus $10,000 Clinical Director pay can drain runway fast if caseloads ramp slowly. The safer sequence is staffing, then room or telehealth load, then expansion once actual sessions match the model.