How do you get clients for a telebehavioral health service?
If you’re trying to get clients for a Telebehavioral Health Service, start with channels you can actually serve: physician referrals, schools, community groups, employers, and behavioral health partners, plus state-specific directories and local SEO. For the KPI side, see What Are The 5 KPIs For Telebehavioral Health Service? and keep growth tied to clinician availability, because the Year 1 model assumes 9,780 monthly treatments and an initial appointment within 48 hours.
Start where demand is real
Build physician referral paths first
Use schools and community groups
Target employers with access needs
List only licensed states
Match marketing to capacity
Credential before payer directory use
Post by specialty and need
Keep intake speed under 48 hours
Do not outrun clinician slots
What are the biggest mistakes starting a telebehavioral health service?
The biggest mistake in a Telebehavioral Health Service is launching before licensure verification, HIPAA workflows, and business associate agreements are in place. Also risky: weak crisis protocols, thin intake, poor documentation, and marketing before provider capacity is ready. Do a readiness gate first and test video access, consent, scheduling, billing, emergency escalation, and documentation before taking patients; if onboarding takes longer than planned, slow acquisition instead of building a waitlist you can’t serve.
Launch risks
Verify licensure before first visit
Sign business associate agreements
Test HIPAA-safe video access
Define crisis escalation steps
Readiness gate
Check consent flow end to end
Test scheduling and billing
Audit documentation before launch
Slow patient acquisition if capacity lags
How long does it take to open a telebehavioral health service?
Opening a Telebehavioral Health Service usually takes 8–20 weeks of planning, and a single-state cash-pay launch can move faster because it skips payer credentialing. Insurance-based, employer-funded, or multi-state launches take longer because they wait on contracting, licensure checks, clinical policy review, and billing workflow testing. Launch month should start only after HIPAA-ready tech, consent forms, emergency protocols, provider schedules, and payment collection are all tested.
Fastest path
8–20 weeks is the planning range
Cash-pay can skip credentialing delays
One state is simpler to launch
Test payment flow before go-live
What slows it down
Insurance adds contracting time
Employer-funded plans need extra review
Multi-state adds licensure checks
Incomplete payer files delay opening
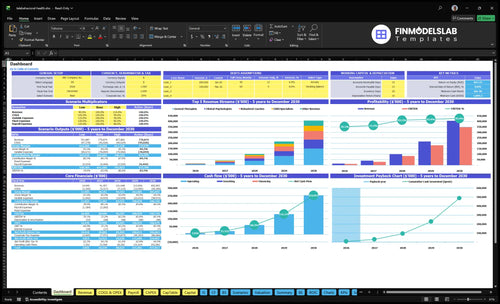
Telebehavioral Health Service Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be complete before accepting patients
Launch readiness checklist
Use this go-live approval checklist to confirm the telebehavioral health service is ready before opening.
1Licensure
State coverage mappedCritical
This confirms where clinicians can treat patients before any intake starts.
Malpractice coverage boundCritical
Coverage should be live before any virtual visit or provider onboarding.
Consent forms approvedHigh
Patients need clear consent before care starts and records are created.
2Clinical flow
Emergency protocol testedCritical
A live crisis plan is needed when a patient is at risk during a session.
Documentation templates readyHigh
Notes must be consistent so care, billing, and audits all line up.
Intake triage definedHigh
Triage keeps the right patient with the right clinician from day one.
3Platform
EHR liveCritical
The record system has to work before any patient chart is opened.
Video visits testedCritical
If video fails, the core service fails, so test it end to end.
Business agreements signedCritical
Data sharing and hosting need signed agreements before patient data flows.
4Providers
Clinicians credentialedCritical
Only approved clinicians should see patients and bill for care.
Onboarding completeHigh
New providers need training on workflow, records, and escalation steps.
Capacity matches forecastHigh
Headcount should match the forecasted volume in the first year.
5Revenue
Scheduling worksCritical
Patients need a clean path to book, reschedule, and show up.
Billing path testedCritical
Revenue cannot start until claims or invoices move without breaks.
Referral sources readyMedium
Referral channels matter once intake opens and the first demand push starts.
6Finance
Runway covers launchCritical
Minimum cash is $1.004m in Month 1, so launch needs that cushion funded.
Revenue ramp reviewedHigh
The model should tie provider capacity, pricing, and visit volume to revenue.
Go-live signoff completeCritical
Final signoff should confirm compliance, workflow, tech, and cash are ready.
Which launch drivers decide if you can safely open?
1State Licensure
State matrix
A state-by-state license matrix is the launch gate before scheduling begins.
2HIPAA Tech
Tested flow
A tested booking-to-payment flow cuts failed visits and protects documentation before launch.
3Clinical Workflow
1 mock visit
A mock visit proves intake, consent, note, and follow-up steps work.
4Provider Staffing
35-50% cap
Year 1 capacity spans 35% to 50%, so demand must not outrun staffing.
5Billing Ready
30% fees
Billing setup controls cash timing and cuts rework after the first visit.
6Patient Acquisition
100% rev
A channel plan tied to provider hours avoids wasted spend and poor conversions.
State Licensure and Compliance
State Licensure and Compliance
Opening depends on whether each patient’s location matches a clinician’s active license. A single gap in the state-by-state clinician matrix can block patient acceptance in that state, even when demand is strong. For a service promising an initial visit within 48 hours, licensure checks have to be done before scheduling starts.
This driver also covers consent, privacy under HIPAA, documentation, malpractice coverage, and emergency protocols. If you plan multi-state care, the bottleneck risk rises fast, because launch is only as open as the weakest state on the matrix.
Verify before booking
Build the state-by-state clinician matrix first, then confirm every active state has a licensed provider, the right practice scope, and a clear escalation path. Route intake only after each state is approved so first-day scheduling does not outrun compliance.
Check each board’s license status.
Review interstate practice rules.
Set consent and HIPAA documents.
Confirm malpractice coverage.
Map crisis escalation contacts.
Use a hard launch gate: if one state is unverified, that state stays closed. That keeps the team from fixing compliance after bookings start, which can delay first revenue and force manual work on day one.
1
HIPAA-Ready Technology
HIPAA Tech Stack
If the tech stack isn’t HIPAA-ready, you can’t open cleanly. Secure video, scheduling, EHR, intake forms, documentation, messaging, billing integration, and business associate agreements (BAAs) all need to work together before the first booking. The readiness signal is one tested patient journey from booking through payment and chart note.
That matters because weak permissions, vendor gaps, or missing agreements can stall launch even when demand is there. The Year 1 model already assumes HIPAA cloud hosting at 30% of revenue, so setup choices hit cash fast. One broken link can mean failed visits, messy notes, and avoidable compliance risk.
Test the Full Visit Path
Before opening, map every step from intake to chart close. Verify secure access, role-based permissions, backups, and signed BAAs with each vendor. Then run a mock visit with a therapist, a patient, and billing so you catch broken handoffs before real users do. One test beats ten promises.
Confirm mobile access works.
Check chart note completion.
Test payment after session.
Fix login friction fast.
List the minimum inputs: video tool, EHR, forms, messaging, payment link, support path, and patient login help. If any step takes more than a few clicks or fails on mobile, delay launch or fix it first. The goal is fewer failed visits, cleaner documentation, and safer day-one operations.
2
Clinical Operations Workflow
Day-One Clinical Flow
Opening on time depends on a documented visit path: intake screening, informed consent, scheduling, treatment plans, documentation, no-show policy, crisis escalation, referrals, and discharge. A 48-hour first-appointment promise only works if these steps are already built, trained, and assigned before the first patient books.
Readiness signal: one completed mock visit with intake, session, note, billing, and follow-up. If a patient in crisis would land in a generic inbox instead of a named escalation route, the launch is not safe yet. When staff rely on memory instead of written steps, first-day care breaks fast.
Test the full patient path
Build the workflow in the same order patients feel it: screen, consent, book, treat, document, collect, and close. Then run a mock visit end to end and confirm the note, billing handoff, and follow-up task all happen without manual rescue. One clean test beats ten policy drafts.
Verify intake questions before launch.
Map crisis escalation to a named owner.
Set the no-show rule in writing.
Assign referral and discharge steps.
Check follow-up tasks after every visit.
3
Provider Staffing and Capacity
Clinician Capacity
Opening on time depends on having enough licensed clinicians in the right states, with the right specialties, already onboarded and schedulable. The Year 1 plan assumes 275 providers total: 120 general therapists, 45 clinical psychologists, 20 adult psychiatrists, 30 child specialists, and 60 behavioral coaches. If that mix is not live before launch, the platform can market demand but cannot convert it into appointments.
The risk is simple: more bookings than clinician hours. Year 1 capacity assumptions range from 35% for adult psychiatrists to 50% for behavioral coaches, so the schedule has to match live coverage, not the full roster. If capacity is thin in one specialty, patient wait time rises fast and the 48-hour first-visit promise gets harder to hold.
Lock the roster before opening
Build a state-by-state clinician matrix first, then confirm each clinician’s specialty, availability, supervision setup if needed, and onboarding completion. Test the schedule with a mock week of intake, follow-up, and urgent slots so the team can see where demand will break. One clean rule: do not sell more first visits than the calendar can actually absorb.
Verify state coverage by patient location.
Confirm specialty mix matches demand.
Load appointment templates before launch.
Document quality standards and escalation paths.
Track no-show and refill capacity daily.
4
Payer, Billing, and Payment Readiness
Payer and Billing Setup
Cash-pay can open faster because you can start taking payment on day one. Insurance, hybrid, employee assistance program, or employer-funded models need payer enrollment, credentialing, and billing rules before revenue is real.
This setup has to handle eligibility checks, claims or invoices, payment processing, refunds, and patient balances. The key risk is booking revenue before credentialing is done. That can create cash gaps, payment rework, and a launch that looks open on paper but is not ready to bill.
Lock the billing path before launch
Pick one payment model first, then build the workflow around it. Here’s the quick math: the Year 1 plan already assumes payment processing fees at 30% of revenue, so pricing and cash timing need to be clear before the first visit is booked.
Test the full path from booking to payment to refund handling before go-live. If payer enrollment is still pending, do not count contracted revenue in the launch plan. One clean billing flow matters more than three half-finished ones.
Confirm cash-pay, insurance, or hybrid.
Finish credentialing before scheduling.
Test eligibility, claim, and invoice flows.
Set refund and patient balance rules.
Assign billing owner and escalation steps.
5
Patient Acquisition Channels
Patient Channel Fit
First revenue depends on matching patient channels to the states and specialties your licensed clinicians can actually cover. In Year 1, digital patient acquisition is modeled at 100% of revenue, so marketing into an uncovered state or specialty can waste spend and slow bookings before day one.
One clean target beats five loose ones. A channel plan should map referral partners, directories, local search, payer directories, and employer relationships to available provider hours, so intake can support the promise of an initial appointment within 48 hours.
Build the channel map before spend
Start with a state-by-state list of covered clinicians, then assign each channel to a live service lane. Verify the intake path can capture location, specialty, and urgency fast enough to route patients to a booked slot, not a dead end. If the front door cannot convert, the ad budget becomes stranded cash.
Match channels to licensed states.
Set one niche per launch lane.
Test intake before buying traffic.
Confirm referral handoffs and directory profiles.
The readiness signal is simple: every marketed state must have open provider hours behind it. That keeps first-patient flow cleaner and avoids opening with demand that the schedule cannot absorb.
Start with licensure coverage, HIPAA-ready systems, provider onboarding, clinical policies, billing, and first-patient channels A practical planning range is 8–20 weeks The Year 1 model assumes 275 practitioners, 9,780 monthly treatments at modeled capacity, and $90–$250 treatment prices, so validate capacity before marketing hard
Plan for 8–20 weeks, depending on state licensure, technology setup, staffing, and payer strategy A single-state cash-pay launch can move faster Insurance-based or multi-state launches often take longer because credentialing, contracting, and licensure checks can block opening even when the website and platform are ready
Not always, but you still need compliant operations Confirm state rules, clinician licensing, malpractice coverage, HIPAA policies, consent forms, emergency protocols, and documentation workflows The launch issue is less about the room and more about whether each patient can be served legally, safely, and securely in their state
Credentialing, state licensure checks, HIPAA vendor readiness, and incomplete clinical workflows cause the most common delays If payer files are not complete, insurance revenue may lag If emergency protocols or consent forms are missing, patient acceptance should wait, even if providers and marketing are ready
Book patients only after licensure, intake, consent, video, documentation, billing, and crisis workflows are tested Start with referral partners, provider directories, local search by licensed state, employer channels, or self-pay offers Then compare bookings against provider capacity Year 1 modeled capacity starts at 35%–50% depending on provider type
About the author
Marcus Cole
Business Operations Writer
Marcus Cole is a business operations writer for Financial Models Lab who researches how small businesses launch, operate, and earn money. He focuses on first-year business costs and simple business projections, helping local business owners move from a side project to a real business. His work guides readers from an idea to a basic business plan.
Choosing a selection results in a full page refresh.