Telebehavioral Health Startup Costs: $10M Cash And $480K CAPEX
You’re budgeting a virtual behavioral health launch, so the key issue is not just software cost it’s cash before claims, payroll, and payer setup stabilize This telebehavioral health startup budget includes $480,000 of CAPEX across the startup period, $1004 million of minimum Month 1 cash, and a first-year model outcome of $1494 million revenue with breakeven in Month 1 These are researched planning assumptions, not vendor quotes or guaranteed costs
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for launch; the base setup is $480,000 before contingency.
!
Exclusions This calculator covers capitalized startup assets only. It excludes clinician payroll, advertising spend, insurance premiums, licensing renewals, working capital, deposits, debt service, inventory, and other operating cash needs.
How much money do you need to start a telebehavioral health service?
You need at least $1.004 million in Month 1 cash to start a Telebehavioral Health Service, not just the $480,000 CAPEX, because funding must cover setup costs, pre-opening spend, and working capital; build this into How To Write A Business Plan For Telebehavioral Health Service?. The first-year model also carries $38,200 in monthly fixed costs, $1.025 million in Year 1 wages, and a provider plan of 275 clinicians at 35.0% to 50.0% utilization.
Funding Stack
$480,000 CAPEX base model
$1.004 million minimum Month 1 cash
$38,200 monthly fixed operating costs
$1.025 million Year 1 wages
Scale Drivers
275 Year 1 clinicians planned
General therapists and clinical psychologists
Adult psychiatrists and child specialists
Lean launch cuts platform scope
What hidden costs come up when starting a telebehavioral health service?
Starting a Telebehavioral Health Service means the hidden costs hit cash before revenue does, especially clinician pay before collections, payer enrollment delays, no-show management, and patient acquisition lag; if you track the right KPIs, like in What Are The 5 KPIs For Telebehavioral Health Service?, you’ll spot the drain early. The Month 1 working-capital signal is $1,004 million, and recurring load includes $38,200 in monthly fixed expenses plus about $85,400 in monthly wage run-rate from $1,025 million in Year 1 salaries. Slower collections or lower utilization raise cash need fast.
Cash before revenue
Clinicians get paid before collections.
Payer enrollment can delay reimbursement.
No-show management adds extra labor.
Patient acquisition is 100% digital.
Recurring cost stack
30% payment processing fees.
30% HIPAA cloud hosting.
60% practitioner commission payouts.
Supervision, compliance, and support keep running.
How should founders build a telebehavioral health financial model before raising funding?
Build the Telebehavioral Health Service model from provider capacity, payer mix, collections lag, and startup cash before you raise. Use the Year 1 base case as given: 275 clinicians, $1494 million revenue, $10469 million EBITDA, $480,000 CAPEX, and $1004 million minimum cash. Month 1 breakeven should tie provider counts to monthly treatments, price, and capacity, but treat it as a planning check, not proof of break-even.
Base case inputs
Use 120 providers for general therapists
Map 80 monthly treatments per provider
Test 450% capacity and $120 price
Anchor Year 1 to $1494 million revenue
Stress tests
Delay cash for payer lag
Cut volume for utilization shortfalls
Lower demand for marketing conversion
Slow hires for provider onboarding and state expansion
Calculate Fuding Needs
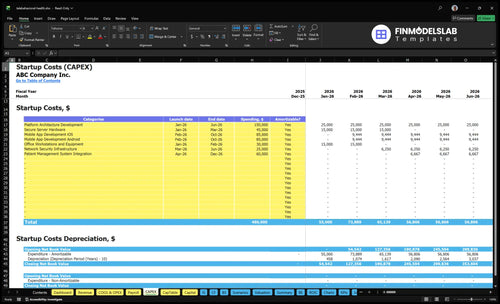
Startup Cost Summary Table
Startup costs cover platform build, app development, core hardware, and opening cash needed before collections catch up.
Highlighted CAPEX$455,000Base planning example
Excluded cash needs$1,004,000Outside CAPEX total
Funding need$1,459,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Platform architecture development
$150,000
Build the core telehealth platform
Yes
Mobile app development
$170,000
Build iOS and Android apps
Yes
Patient management system integration
$60,000
Connect patient workflow systems
Yes
Secure server hardware
$45,000
Buy secure hosting hardware
Yes
Office workstations and equipment
$30,000
Set up staff workstations
Yes
Opening cash buffer
$1,004,000
Month 1 runway for salaries, subscriptions, claims timing, and debt service
No
Telebehavioral Health Service Core Five Startup Costs
Technology Platform and Clinical Software Startup Expense
Platform build cost
A HIPAA-compliant telebehavioral health platform needs secure video, electronic health record (EHR), scheduling, billing, intake, consent, patient portal, analytics, payments, integrations, and e-prescribing if used. The one-time build totals $450,000: $150,000 architecture, $60,000 integration, $45,000 servers, $25,000 network security, and $170,000 mobile app development.
What drives the budget
Price this with vendor quotes, build hours, and module count. Use units × rate for software work, then separate implementation from capitalized build. Recurring source costs are $12,000 a month for platform maintenance and $4,500 for cybersecurity and data protection, or $198,000 a year before cloud hosting. Year 1 also adds 30% HIPAA cloud hosting infrastructure.
How to keep scope tight
Keep the first release focused on clinical basics and compliant workflows. The biggest mistake is paying for custom features before user demand is proven. Start with core scheduling, intake, consent, and payment flows, then layer extras only after launch traffic shows need.
Launch core workflows first
Buy proven integrations
Delay custom reporting
Recurring run rate
The recurring base is $16,500 per month before cloud hosting. That matters because platform costs do not stop at launch; they keep running with support, security, and uptime work, so budget them against expected session volume and data load from day one.
Regulatory, Licensing, Credentialing, and Legal Startup Expense
State rules
Your legal and credentialing spend starts with professional entity setup, state practice rules, clinician license verification, payer credentialing, payer enrollment, HIPAA policies, consent forms, privacy notices, and legal review. If psychiatry is offered, add prescribing rules. Budget by state and provider type; there is no single national license cost. Plan $5,000 per month for ongoing legal and regulatory compliance.
Credentialing labor
Use one Credentialing Specialist at $55,000 annual salary in Year 1 to handle license checks, payer packets, and enrollment follow-up. That role grows with the number of states, providers, and payers. The model reaches 40 FTE by Year 5, so labor is not a one-time setup cost.
Count states served
Count provider types
Count payer enrollments
Cut rework
Keep the $5,000 monthly compliance budget focused on templates and state-specific review, not repeated manual fixes. Start license verification before contracting, and sequence payer credentialing by launch state so clinicians can bill on time. One clean one-liner: slow paperwork is expensive paperwork.
Verify licenses first
Standardize forms once
Launch state by state
Timing risk
State-by-state rules change both budget and timing, so a launch plan should carry separate costs for each state and provider mix. If psychiatry is included, prescribing review adds another layer. The practical watch-out is simple: a fast product launch can still stall if licensing, credentialing, or payer enrollment is not cleared first.
Clinician Recruitment, Onboarding, and Staffing Readiness Startup Expense
Launch staffing
This cost covers recruiting, background checks, license verification, credentialing packets, onboarding time, supervision setup, clinical protocols, documentation training, crisis workflows, and a launch payroll reserve. The Year 1 provider network assumes 275 clinicians: 120 therapists, 45 psychologists, 20 adult psychiatrists, 30 child specialists, and 60 behavioral coaches.
Estimate it
Model this with headcount times hiring steps, plus onboarding hours times loaded pay, plus the weeks of payroll needed before sessions ramp. Keep one-time onboarding separate from ongoing clinician pay and commission payouts. The internal team adds 9 staff, and the source lists $1025 million in Year 1 wages across those roles.
Batch license checks by state.
Standardize credentialing packets.
Track reserve weeks before launch.
Cut waste
Lower this cost by staging hires, reusing training modules, and delaying any specialty onboarding until demand is visible. Do not skip crisis workflow training or documentation review; that creates rework and compliance risk. One clean rule: hire to booked capacity, not to a hoped-for waitlist.
Hire in waves, not all at once.
Use recorded training for basics.
Keep supervision setup uniform.
Cash timing
Separate the one-time onboarding spend from steady clinician compensation. If launch slips, the payroll reserve still burns while recruiting, verification, and credentialing keep running. The real test is not just filling 275 clinician slots; it’s paying for the gap between hire date, first booked session, and full network use.
Insurance and Risk Management Startup Expense
Policy stack
Your telebehavioral health risk budget needs more than malpractice. A realistic stack includes professional liability, cyber liability, general liability, workers’ compensation, and directors and officers cover if you raise capital. Add policy deposits and match claims limits to each provider class and state.
Price drivers
Use provider mix, service scope, and state count to price it. The source data puts recurring professional liability at $6,000 per month and cybersecurity and data protection at $4,500 per month. Premiums shift with adult psychiatry, child specialist coverage, prescribing, claims history, provider count, and the limits you buy.
Tighten spend
Get quotes by state and by provider type, not one national average. Keep the active states and clinician mix tight, and only add higher limits when contracts, prescribing, or fundraising require them. That keeps the premium base tied to actual exposure instead of planned expansion.
Coverage map
For a teletherapy platform, the policy file should show coverage by provider type and state, plus limits for malpractice, cyber, general liability, workers’ compensation, and any D&O cover. Price each line off current headcount, license map, prescribing rights, and claims history, then refresh after each new state launch or capital round.
Launch Marketing, Patient Acquisition, and Channel Setup Startup Expense
Launch spend
Telebehavioral health launch marketing is a pre-opening expense, not CAPEX. Budget for website build, SEO setup, state or local landing pages, paid search tests, referral outreach, employer and payer materials, launch brand assets, and conversion tracking. Estimate it from channel count, page count, and months of test spend. One line: if you can’t track leads, you can’t price growth.
Year 1 math
Use patient acquisition as a revenue-linked cost. The model says variable digital acquisition is 100% of revenue in Year 1, then 70% by Year 5. Add the marketing team cost too: $95,000 for one Marketing Manager in Year 1, with staffing rising from 10 FTE to 30 FTE by Year 5.
Price by channel, not guesswork
Track cost per booked visit
Match spend to filled capacity
Spend control
Keep early spend tight by testing one or two paid channels, using local landing pages, and sending referral and employer outreach to the same tracked funnel. The goal is not broad awareness; it’s booked sessions. If provider schedules are thin, cut acquisition until capacity fills, since empty slots burn cash fast.
Start with trackable channels only
Use payer mix in the budget
Expand after fill rates improve
Channel fit
Budget should follow payer mix, provider availability, and fill rate. If the platform can’t book enough visits within 48 hours, more marketing just pushes unfilled demand. Tie each dollar to a source, a booked appointment, and a live clinician slot so you know when to scale and when to pause.
Compare 3 Startup Cost Scenarios
Scenario comparison
Costs rise fast as you add clinicians, states, payer setup, app scope, and compliance. Lean, base, and full launches help match cash need to real scope.
Lean, base, and full launch cost bands for a telebehavioral health service.
Scenario
Lean LaunchLean scope
Base LaunchModeled launch
Full LaunchScale launch
Launch model
Single-state, provider-led launch with limited customization and a narrow payer setup.
Multi-provider launch that matches the modeled base case across core therapy and psychiatry services.
Multi-state platform launch with broader credentialing, payer contracting, and psychiatry support.
Typical setup
Use one core platform build, basic mobile access, and a small clinician panel.
Build the standard platform, cover the main clinician mix, and run full support and compliance.
Expand state-by-state coverage, deepen integrations, and keep a larger cash buffer.
Cost drivers
Lower custom build
limited payer setup
basic mobile app scope
lighter compliance load
shorter runway
Base platform build
standard payer mix
normal marketing scope
core EHR integration
modeled working capital
Multi-state credentialing
payer contracting
deeper EHR integration
larger marketing spend
longer cash reserve
Planning rangeCAPEX only
$250,000 - $400,000Lean band
$480,000 - $1,004,000Base band
$900,000 - $1,800,000Full band
Best fit
Fits founders testing one state, one care model, and tighter cash control.
Fits teams launching the full modeled service set without multi-state complexity.
Fits operators building for faster scale across states and more care lines.
!
Planning note: Scenario ranges are researched planning assumptions from the model; they are not exact vendor quotes or guaranteed bids.
Not necessarily, but you still need an operating base for administration, security, and clinical governance The model includes $8,500 per month for administrative office space, plus $4,500 for cybersecurity and $12,000 for platform maintenance If you run fully remote, reduce the office line only after confirming state rules, payer requirements, and staff workflow needs
They can be in some models, but classification depends on state rules, payer contracts, control over work, and supervision standards This model uses practitioner commission payouts at 60% of revenue in Year 1, declining to 40% by Year 5 It also carries $1025 million in Year 1 employee wages for leadership, engineering, support, credentialing, and marketing
It affects cash flow until enrollment, documentation, claims submission, and collections are working smoothly The model does not give a credentialing timeline, so treat delays as a working-capital risk, not a one-time setup cost The key reserve is $1004 million minimum Month 1 cash, alongside 100% digital acquisition and 30% payment processing in Year 1
Budget enough runway to cover fixed costs, payroll, variable costs, and collection delays if utilization lags The modeled business reaches breakeven in Month 1 with $1004 million minimum cash, but that depends on first-year capacity assumptions of 350% to 500% by provider type Monthly fixed costs start at $38,200, and Year 1 wages total $1025 million
Model state costs as separate drivers for licensing, credentialing, legal review, insurance, marketing pages, and compliance maintenance Platform CAPEX may not rise one-for-one by state, but complexity can still grow through integrations and workflows The base model includes $60,000 for patient management integration, $25,000 for network security, and $170,000 for combined mobile app development
About the author
Marcus Cole
Business Operations Writer
Marcus Cole is a business operations writer for Financial Models Lab who researches how small businesses launch, operate, and earn money. He focuses on first-year business costs and simple business projections, helping local business owners move from a side project to a real business. His work guides readers from an idea to a basic business plan.
Choosing a selection results in a full page refresh.