How To Start A Telemedicine Business In 8 To 20 Weeks
To start a telemedicine business, build the care model first, then match it to licensed providers, privacy workflows, malpractice coverage, patient consent, scheduling, billing, and support A practical launch window is often 8 to 20 weeks, depending on state coverage, provider onboarding, credentialing, and platform setup In the researched planning case, Year 1 starts with 13 clinicians and about 753 monthly visits at 20% to 40% capacity First revenue usually comes from cash-pay visits, employer or referral channels, or focused care packages
Time to Open6 monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepPaid consultsCash-pay live
Launch timeline
This is a short web summary; the XLSX export contains the detailed Gantt chart.
Confirm what must be ready before accepting telemedicine patients
Launch readiness checklist
Use this go-live approval checklist before opening the telemedicine service to confirm compliance, care flow, and cash readiness.
1Compliance
Entity formedCritical
The service needs one legal entity before contracts, payables, and claims start.
State licenses mappedCritical
Coverage by state must be clear before any patient books.
Malpractice coverage boundCritical
Coverage should be active before providers see the first patient.
2Clinical rules
Care protocols approvedCritical
Scripts for common visits keep care consistent and safe.
Escalation path testedCritical
Urgent cases need a live handoff path before launch.
E-prescribing workflow approvedHigh
If used, the prescription path must work with pharmacy rules.
Documentation template lockedHigh
Visit notes need a fixed format for records and follow-up.
3Platform
Booking flow testedCritical
A patient must be able to book without manual help.
Consent forms liveCritical
Consent has to be captured before the visit starts.
HIPAA controls verifiedCritical
Health Insurance Portability and Accountability Act (HIPAA) controls must protect patient data.
4Patient flow
Intake form completeHigh
History, symptoms, and contact data must be ready before booking.
Video visit stableCritical
The visit should work on phone and video with no dropouts.
Follow-up path setHigh
Patients need docs and next steps after the call.
5Staffing
Providers onboardedCritical
Each clinician needs onboarding before schedules open.
Support desk staffedHigh
Patients need a live help path for booking and aftercare.
Shift schedules publishedHigh
Coverage must match demand before the first launch week.
6Revenue
Pricing approvedHigh
Rates must cover payouts, fees, and overhead.
Payment capture testedCritical
A patient should pay before or at the visit.
Billing workflow validatedCritical
Billing must post cleanly or cash will slip.
Cash runway checkedCritical
The model shows a $661k minimum cash need at Month 12.
Go-live signoff completeCritical
Final signoff should confirm every launch gate is green.
Want to see the six launch drivers that matter most?
1Compliance Strategy
8-20 wks
State licenses, consent, and prescribing rules decide where you can launch and which visits clear.
2Provider Network
13 clinicians
Year 1 needs 13 clinicians across specialties so calendars can absorb booked demand.
3HIPAA Tech
Mock flow
Patients must book, pay, join, and get follow-up without workflow breaks or abandoned visits.
4Patient Acquisition
753 visits/mo
Year 1 assumes 753 monthly visits, so the first channel must create booked consultations, not just leads.
5Billing Model
$75-$150
Cash-pay, insurance, or hybrid billing must collect cleanly, or the first month leaks revenue.
6Ops Escalation
Day 1 QA
Support, triage, and escalation rules keep safe visits from failing after booking.
Why test a Telemedicine launch plan before go-live?
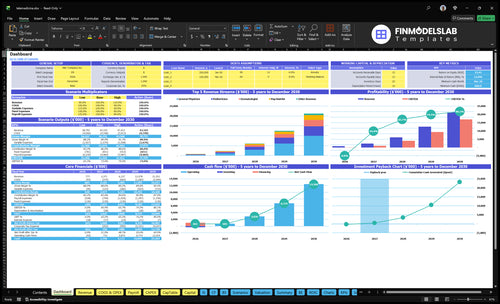
The dashboard shows charts, tabs, and assumption tables for timing, ramp, capacity, staffing, pricing, spend, runway, and breakeven—open the Telemedicine Financial Model Template.
Launch model highlights
13 clinicians planned
753 monthly visits
$75 to $150 pricing
110% payout load
50% acquisition spend
Runway and breakeven
What are the requirements to start a telemedicine business?
To start a Telemedicine business, you need state-matched provider licenses, HIPAA-compliant privacy controls, patient consent, prescribing rules, malpractice coverage, and safety workflows before taking the first patient; the key metric to watch is covered here: What Is The Most Important Indicator Of Success For Telemedicine?. Requirements vary across the 50 US states and by service type, so get legal and clinical review before offering 24/7 non-emergency care.
Must-have setup
Define covered non-emergency services
Pick launch states first
Use licensed clinicians per patient location
Document scope, consent, and protocols
Launch controls
Configure secure intake and visits
Follow HIPAA privacy rules
Check prescribing and malpractice coverage
Test billing before patient volume
How long does it take to start a telemedicine business?
If you’re starting Telemedicine, plan on 8 to 20 weeks to get live. A lean cash-pay launch can move faster, but a multi-state payer-based rollout usually takes longer because of state coverage, provider recruiting, credentialing, platform setup, payer enrollment, policies, and testing. The biggest delays are usually licensing gaps, missing provider documents, consent workflow issues, and billing setup.
Faster launch path
Start with one state
Use cash-pay first
Recruit ready providers
Keep the workflow simple
Common delays
Licensing gaps slow launch
Incomplete provider docs stall credentialing
Consent issues break testing
Billing setup adds time
How do you get first telemedicine patients?
To get first Telemedicine patients, start with channels that can book now, not broad awareness. The best early bets are cash-pay visits, niche condition campaigns, employer wellness partnerships, local provider referrals, urgent-care overflow, and membership packages, because the year-one model needs about 753 monthly visits. Before spending, make sure the landing page, trust signals, appointment slots, payment flow, intake, consent, and follow-up are ready, and use What Is The Estimated Cost To Open And Launch Your Telemedicine Business? to pressure-test setup costs.
Best first channels
Cash-pay visits close fastest.
Niche campaigns target one condition.
Urgent-care overflow fills open slots.
Local referrals bring trusted patients.
Readiness checks
Landing page must explain the offer.
Trust signals should be easy to see.
Payment flow must be simple.
Follow-up should happen fast.
Key Takeaways
Licenses and policies must match each launch state.
Provider capacity has to meet booked demand.
Workflow tests should cover booking through follow-up.
Pricing and operations must be ready on day one.
Compliance And Licensing Strategy
Licensing and State Access
Telemedicine can't open cleanly until patient location, provider licenses, and service type line up. If a patient is in a state where the clinician is not licensed, that visit can be blocked, which hurts day-one revenue and creates a bad first experience.
The readiness test is simple: each launch state needs matched clinicians, written clinical workflows, and patient-facing consent that covers privacy, prescribing, and care limits. If you expand into a state before those pieces are ready, you may still be open on paper but unable to treat patients in practice.
Launch-state checklist
Before opening, map each target state to a licensed clinician, the allowed visit types, and the exact consent shown before booking. Then test the full flow: location check, intake, consent, visit, and any prescription step. That’s how you cut blocked visits and avoid rework after launch.
Match clinicians to each state
Document telehealth workflows
Confirm patient consent screens
Review prescribing limits
Keep privacy steps consistent
What this hides: if licensing or policy review slips, marketing can still bring in demand, but operations won’t be able to serve it. That turns early traffic into delays, refunds, and support load instead of completed visits.
1
Provider Network Readiness
Provider Network Readiness
This launch driver controls whether telemedicine can open on time. With a Year 1 plan for 13 clinicians — 5 general physicians, 3 pediatricians, 2 dermatologists, 2 psychiatrists, and 1 nutritionist — the business needs licensed coverage in target states before marketing turns on.
If calendars are not loaded and staffed by specialty, demand will outrun supply on day one. That creates long waits, missed consults, and weaker patient trust, even if the platform itself works. The readiness test is simple: licensed clinicians, open appointment slots, matching documentation standards, and service levels that can absorb first-week bookings.
Lock Calendars Before Demand
Verify each clinician’s state license, specialty coverage, and booked hours before launch. Build the schedule around the smallest capacity first, not the biggest hope. One overloaded specialty can slow the whole launch, especially psychiatry and dermatology if demand spikes early.
Set one shared intake and charting standard so every visit is documented the same way. Then test whether a mock patient can book, join, and finish a consult without manual fixes. If marketing starts before the provider calendar is full, first consultations slip and the opening date looks real on paper but not in practice.
Match licenses to target states.
Load calendars before ads run.
Standardize documentation across clinicians.
Cover each specialty at launch.
Test first consult flow end to end.
2
HIPAA-Ready Technology And Workflows
HIPAA-Ready Workflow
For telemedicine, the launch is only ready when the full patient flow works end to end: video visits, scheduling, intake forms, consent capture, secure messaging, documentation, payment collection, and support tickets. If any step breaks, patients drop off and staff end up fixing gaps instead of seeing patients. One clean flow protects protected health information (PHI) and keeps day-one care moving.
The key risk is buying software but not wiring the workflow. A mock patient should be able to book, complete forms, pay, join the visit, receive follow-up, and trigger support without manual rescue. If that test fails, opening slips, records get messy, and first-day revenue gets delayed because visits stall before they start.
Test the full patient path
Before opening, run the whole journey with staff: book the visit, send intake, capture consent, process payment, start the call, send the note, and open a support ticket. If one handoff needs a workaround, fix it now and document the step. That is how you avoid launch-day confusion and keep clinicians on schedule.
Assign one owner for each handoff: scheduling, clinical intake, billing, and support. Also check that forms, messaging, and visit notes land in the right place every time. Here’s the quick rule: if a patient can’t finish the flow alone in one test, the launch is not ready.
Verify booking to follow-up flow
Test payment before visits start
Document escalation and support steps
Confirm clean records after each visit
3
Patient Acquisition Channel
Patient Acquisition Readiness
For telemedicine, this launch driver decides whether patients show up on day one. You need a clear niche, one patient problem, trust signals, referral sources, state targeting, and a landing page that makes booking easy. If those pieces slip, the service may open on paper but still sit idle.
The Year 1 model assumes 753 monthly visits, or about 25 visits per day, so the channel has to drive booked consultations, not just leads. A first channel that can produce cash-pay, employer, referral, or focused-care demand is what speeds revenue validation. No bookings, no real launch.
Test One Channel Before Go-Live
Pick one state, one audience, and one offer first. Build the landing page with the condition, price, provider credentials, consent, and a simple book-now path. Then test the full flow: visit, form, payment, scheduling, and confirmation. If any step breaks, launch timing slips.
Track booked consults, not clicks.
Use one niche and one state.
Show trust signals up front.
Measure conversion daily.
If traffic comes in but appointments do not, fix the offer, trust cues, or referral source before adding spend. A weak channel can burn cash fast, while a clean channel helps the business start serving patients and collecting revenue from the first week.
4
Billing, Pricing, And Revenue Model
Billing Model Setup
Pick the billing model before launch, because it sets how every visit gets paid, coded, and receipted. For telemedicine, that means choosing cash-pay, insurance, employer contracts, subscriptions, or a hybrid model before the first patient books. If this is still open, staff can’t quote prices, collect correctly, or process refunds without delays.
Year 1 pricing assumptions are $75 general physician, $85 pediatrician, $100 dermatologist, $150 psychiatrist, and $90 nutritionist. The readiness signal is simple: payment collection, claims workflow if used, refund policy, coding, and patient receipts are all tested. When that path works, revenue leaks drop in the first operating month.
Test the Payment Path Early
Treat billing as a launch gate, not a post-launch cleanup job. Map one payment path for each visit type, then test it with a mock patient from booking to receipt. If insurance is part of the model, the claims workflow must be live before opening. If not, cash collection and refund handling still need a clean script.
Confirm each service price.
Test card capture and refunds.
Verify claims only if used.
Issue receipts after every visit.
Assign one owner to billing rules, one to coding, and one to support disputes. A broken price table or missed receipt on day one slows cash, confuses patients, and creates avoidable rework before the first month closes.
5
Operations, Quality Control, And Escalation
Day-One Escalation Control
This driver decides whether booked visits actually turn into safe care. If the team cannot tell, on day one, who handles a tech issue, urgent symptom, missed visit, or payment dispute, the platform can still fail after booking. That creates early churn, complaint spikes, and avoidable clinical risk.
With a provider mix sized for 5 general physicians, 3 pediatricians, 2 dermatologists, 2 psychiatrists, and 1 nutritionist, the real bottleneck is not demand. It is whether support, triage, QA, and documentation checks keep each visit moving and each escalation in the right hands. For a 24/7 model, missed handoffs hit trust fast.
Test the worst cases before launch
Before opening, run the full patient flow: booking, intake, consent, payment, visit join, follow-up, and ticket handoff. Write the clinical triage and urgent escalation rules, assign a back-up owner for no-shows, and set a simple complaint and service recovery log so staff know exactly what happens next.
Mock a tech failure and payment dispute.
Check documentation before release.
Review provider notes for QA.
Train support on urgent handoffs.
A good readiness signal is simple: a new patient can get help without staff improvising. The team should know who answers, who escalates, who documents, and who follows up when a visit is missed or a symptom sounds urgent.