7 Critical Financial KPIs for Primary Care Clinic Growth
KPI Metrics for Primary Care Clinic
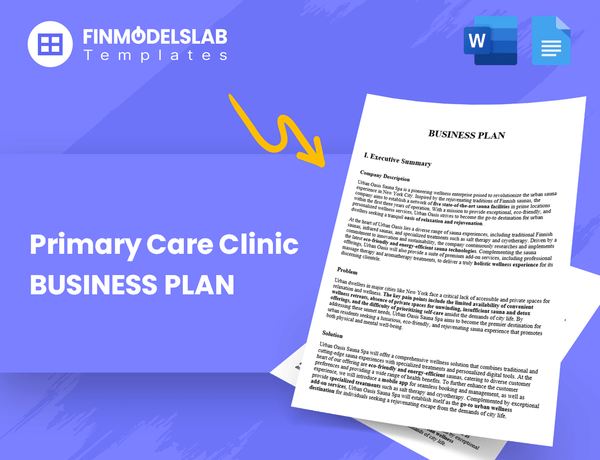
To ensure your Primary Care Clinic scales profitably, you must track seven core financial and operational KPIs, focusing heavily on provider efficiency and collection rates We see a strong need to hit breakeven by January 2027 (Month 13), requiring tight control over capacity utilization, which starts low at 600% for GPs in 2026 Key metrics include Revenue Per Visit, Gross Margin (targeting 90%+), and Provider Utilization Rate, reviewed weekly
7 KPIs to Track for Primary Care Clinic
#
KPI Name
Metric Type
Target / Benchmark
Review Frequency
1
Provider Utilization Rate
Capacity Metric
Aim for 850% utilization by 2030 (starting at 600% in 2026)
Monthly
2
Revenue Per Visit (RPV)
Financial Metric
Target $131 weighted average RPV based on 2026 projections
Monthly
3
Gross Margin Percentage
Profitability Metric
Must exceed 90% to cover $12,000 fixed monthly rent
Monthly
4
Patient Acquisition Cost (PAC)
Efficiency Metric
Track closely; marketing spend is currently budgeted at 30% of revenue
Monthly
5
Operating Expense Ratio (OER)
Efficiency Metric
Must drop sharply from Year 1 to achieve $341,000 Year 2 EBITDA
Quarterly
6
Months to Breakeven
Milestone Metric
Must reach this point by January 2027 (13 months) to manage cash runway
Monthly
7
Working Capital Cycle
Liquidity Metric
Minimize cycle time due to high 50% Billing & Collections Fees
Monthly
Primary Care Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What are the primary drivers of revenue and how quickly can we scale them?
The primary revenue drivers for the Primary Care Clinic are the number of active General Practitioners (GPs) and the utilization rate, targeting 160 treatments per GP monthly by 2026; scaling hinges defintely on adding providers, moving from 2 GPs in 2026 to 5 by 2030, so understanding your capacity limits is key, especially when Are You Tracking The Operational Costs Of Primary Care Clinic Regularly?
Provider Capacity Growth
Capacity starts with 2 GPs scheduled for 2026.
Goal is to reach 5 GPs on staff by the year 2030.
This growth dictates the maximum achievable service volume.
If onboarding takes 14+ days, churn risk rises.
Monthly Treatment Targets
Each provider must hit 160 treatments monthly in 2026.
This volume assumes successful patient scheduling and utilization.
Revenue is strictly fee-for-service per consultation.
The model relies on optimized capacity management.
How efficient are our providers and support staff relative to industry benchmarks?
Efficiency for the Primary Care Clinic hinges on tracking capacity utilization, especially for new roles like Dietitian and Counselor, which project an aggressive 400% utilization in 2028. This metric dictates staffing needs and revenue scaling, which directly impacts how much the owner makes, as detailed in analyses like How Much Does The Owner Make From A Primary Care Clinic?
Measure Provider Capacity
Standard primary care utilization benchmarks hover around 75% to 85% of available appointment slots filled.
For the Primary Care Clinic, track billable time versus scheduled provider time monthly.
Support staff utilization must track provider load; if providers are 80% utilized, support staff should mirror that efficiency.
Benchmark new service utilization against established roles to spot immediate scaling issues.
Analyze Extreme Utilization
A 400% utilization target for Dietitian and Counselor services in 2028 needs immediate clarification.
This suggests the model counts four patient interactions for every hour available, which is defintely not standard provider time.
If this high number is accurate, it implies a highly efficient group model or a misunderstanding of the metric definition.
If onboarding takes 14+ days, churn risk rises before these new services hit peak capacity.
What is the true cost of delivering a single patient visit, including all overhead?
The true cost of delivering a single patient visit for the Primary Care Clinic is significantly negative because total variable costs exceed 100% of revenue based on the specified cost structure. Specifically, variable expenses total 160% of revenue, yielding a contribution margin of negative 60%. If you're looking at how much the owner might make in a sustainable model, check out How Much Does The Owner Make From A Primary Care Clinic?
Variable Cost Drivers
Medical Supplies (COGS) account for 35% of revenue.
Lab Fees (COGS) account for 45% of revenue.
Billing Fees (Variable OpEx) consume 50% of revenue.
Marketing (Variable OpEx) consumes 30% of revenue.
Margin Reality Check
Total variable costs sum to 160% of revenue.
The resulting contribution margin is negative 60%.
You defintely cannot cover any fixed overhead costs this way.
You must cut variable costs by 60% just to reach zero contribution.
When do we achieve operational breakeven and what is the required patient volume?
The Primary Care Clinic is projected to hit operational breakeven in January 2027, which is 13 months after launch. This milestone depends entirely on achieving the necessary patient volume to offset $20,100 in fixed monthly overhead, including staff wages, and you're defintely going to need tight control over scheduling to hit that target. The required volume calculation determines if the Primary Care Clinic is currently achieving sustainable profitability, which you can review here: Is The Primary Care Clinic Currently Achieving Sustainable Profitability?
Fixed Cost Coverage
Monthly fixed costs, which include wages, stand at $20,100.
Breakeven requires patient volume to generate revenue covering this amount.
The target date for reaching this stability is January 2027.
This timeline assumes no major unexpected capital expenditures arise.
Volume Levers
Revenue comes from a fee-for-service model per consultation.
High utilization rates are key to covering the $20,100 fixed base.
Optimized capacity management directly drives service delivery volume.
If practitioner workloads aren't balanced, volume growth stalls quickly.
Primary Care Clinic Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Key Takeaways
Achieving the January 2027 breakeven milestone is paramount to successfully managing the initial projected $558,000 cash burn before sustained profitability.
The primary driver for financial health is immediately boosting Provider Utilization Rate from the starting 600% to effectively cover high fixed operating expenses.
The clinic must rigorously target a Gross Margin Percentage exceeding 90% to ensure sufficient revenue remains after direct costs to absorb significant overhead like $12,000 monthly rent.
Due to the high initial 50% cost allocated to Billing & Collections Fees, tight management of the Working Capital Cycle is crucial for optimizing cash flow velocity.
KPI 1
: Provider Utilization Rate
Definition
Provider Utilization Rate shows how much of your available practitioner time you are actually using to deliver billable treatments. This metric is vital because your primary cost driver—your physicians’ salaries—is largely fixed, so maximizing their productive time directly impacts profitability. For your clinic, this measures success in balancing patient demand against your optimized capacity system.
Advantages
Maximizes revenue capture from fixed provider salaries and overhead costs.
Allows you to spread high fixed expenses, like the $12,000 monthly rent, across more services.
High utilization signals that your capacity management system is working as planned.
Disadvantages
Unsustainable utilization levels lead directly to provider burnout and turnover.
It can mask poor quality if providers rush appointments to hit volume targets.
Leaves no buffer time for complex cases or unexpected administrative needs.
Industry Benchmarks
In typical primary care settings, utilization often targets 70% to 90% of scheduled time, assuming a standard 40-hour week. Your plan to start at 600% in 2026 and reach 850% by 2030 suggests you are defining capacity very narrowly, likely counting only direct patient interaction time against a very low theoretical maximum. These aggressive targets mean operational excellence is not optional; it’s baked into your growth plan.
How To Improve
Optimize scheduling blocks to minimize transition time between patients.
Implement automated reminders to drive down patient no-show rates.
Increase the average Revenue Per Visit (RPV) so fewer treatments are needed for the same revenue.
How To Calculate
You calculate this by dividing the number of treatments actually delivered by the maximum number of treatments your providers could theoretically handle in that period. This ratio shows how effectively you are monetizing your provider base.
Provider Utilization Rate = Actual Treatments / Max Capacity
Example of Calculation
Using your 2026 projection, if your maximum theoretical capacity is based on 402 actual treatments, hitting 600% utilization means you need to deliver 2,412 treatments that month. Here’s the quick math: (2,412 Actual Treatments / 402 Max Capacity) = 6.0, or 600%. This calculation hinges entirely on how rigorously you define that denominator.
Tips and Trics
Segment utilization by provider; one low performer drags down the whole average.
If utilization is too high, immediately review provider compensation structure to prevent burnout.
Track utilization against the $131 RPV target; low utilization with high RPV is better than high utilization with low RPV.
Defintely review your scheduling software integration quarterly to ensure no data leakage.
KPI 2
: Revenue Per Visit (RPV)
Definition
Revenue Per Visit (RPV) is the average dollar amount earned for every medical treatment or consultation delivered. This metric directly reflects your pricing strategy and the mix of services you sell. For the clinic in 2026, the weighted average RPV is ~$131 based on $52,560 in revenue divided by 402 actual treatments.
Advantages
Shows true value captured per patient interaction.
Helps analyze if high-value procedures are being prioritized.
Acts as an early warning if discounting erodes per-visit profitability.
Disadvantages
It masks the underlying volume needed to hit revenue targets.
It doesn't account for the cost associated with delivering that visit.
It can be skewed by the 50% Billing & Collections Fees if collections lag.
Industry Benchmarks
Primary care RPV varies widely based on payer mix and service depth. High RPV often suggests a focus on complex chronic care management or high-fee procedures, rather than simple preventative visits. Benchmarking against similar fee-for-service models helps confirm if $131 is competitive for your service scope.
How To Improve
Increase the percentage of high-reimbursement procedures included in the standard visit.
Negotiate better rates with key insurance carriers to increase the fee captured per service code.
Bundle preventative screenings into the initial consultation fee rather than billing them separately later.
How To Calculate
RPV is calculated by dividing your total monthly revenue by the total number of treatments provided that month. This gives you a clear dollar figure for every interaction.
Example of Calculation
To find the 2026 weighted average RPV, you divide the total revenue by the total treatments delivered. Here’s the quick math:
$52,560 / 402 treatments
equals $131.24 per visit. This figure is the baseline for measuring pricing effectiveness.
Tips and Trics
Track RPV segmented by provider to spot training needs.
Review RPV monthly against the target of $131.
Ensure revenue recognition matches service date, not payment date.
Watch for RPV dips when marketing brings in many new, low-complexity patients.
KPI 3
: Gross Margin Percentage
Definition
Gross Margin Percentage shows how much revenue remains after paying for the direct costs of providing care. This metric is crucial because it determines your ability to cover fixed expenses, like the $12,000 monthly rent. If this number is too low, you’re running a service business that can’t afford its own building.
Advantages
Directly measures pricing power against variable service inputs.
Shows immediate profitability before overhead hits the books.
A high margin provides a necessary buffer against unexpected cost increases.
Disadvantages
It completely ignores fixed overhead costs like rent and salaries.
A high margin doesn't guarantee positive EBITDA if volume is too low.
It can mask poor operational efficiency if supply costs are subsidized temporarily.
Industry Benchmarks
For specialized healthcare services, Gross Margin Percentage benchmarks vary widely based on payer mix and service complexity. However, given the $12,000 fixed overhead, this clinic needs a margin well above standard retail service models. A target of 90%+ is required to ensure sufficient contribution margin flows down to cover those high fixed costs.
How To Improve
Aggressively renegotiate Medical Supplies costs currently set at 35% of revenue.
Find ways to reduce Lab Fees, which consume 45% of revenue, perhaps through in-house testing agreements.
Increase Revenue Per Visit (RPV) by ensuring every patient receives appropriate, billable services.
How To Calculate
Calculate Gross Margin Percentage by taking total revenue, subtracting the cost of goods sold (direct costs), and dividing that result by total revenue. You must track Medical Supplies and Lab Fees as your primary direct costs.
If monthly revenue hits $100,000, and direct costs are 35% for supplies ($35,000) and 45% for labs ($45,000), your total direct cost is $80,000. This leaves a 20% margin, which is not enough to cover overhead. To hit the 90% target, direct costs must only be 10% of revenue, meaning you need to cut $70,000 in current projected direct spending.
Track supply costs as a percentage of revenue daily, not just monthly.
If Lab Fees exceed 45% for two consecutive weeks, flag it for immediate renegotiation.
Ensure RPV growth consistently outpaces any inflation in supply costs.
The 90% target is defintely the minimum required contribution margin floor.
KPI 4
: Patient Acquisition Cost (PAC)
Definition
Patient Acquisition Cost (PAC) is the total marketing dollars spent divided by the number of new patients you brought in that month. It measures how much it costs, on average, to secure one new relationship. For this clinic, marketing is budgeted as a fixed 30% of Revenue, making PAC highly sensitive to top-line performance.
Advantages
Links marketing investment directly to patient growth volume.
Helps assess if marketing spend is scalable before major expansion.
Allows comparison against the projected Lifetime Value (LTV) of a patient.
Disadvantages
If marketing is 30% of revenue, PAC automatically inflates as revenue grows, even if efficiency is flat.
It can hide poor performance if revenue spikes due to high service prices (high RPV).
It doesn't account for the cost of converting a lead into a patient (sales effort).
Industry Benchmarks
Benchmarks for primary care acquisition vary based on whether you are targeting new patient volume or specialized chronic care management. For community-based models, a PAC under $250 is generally sustainable if the patient stays for several years. You want this number defintely lower than the first year's expected revenue contribution per patient.
How To Improve
Shift marketing budget from percentage-of-revenue to fixed dollar targets based on capacity.
Prioritize referral programs to leverage existing patient satisfaction for zero-cost acquisition.
Increase Provider Utilization Rate to maximize revenue from existing patient flow.
How To Calculate
You calculate PAC by taking your total monthly marketing expenditure and dividing it by the number of new patients who signed up that same month. The key risk here is that the marketing spend is tied to revenue, not just patient count.
PAC = Marketing Spend / New Patients Acquired
Example of Calculation
Using the reported 2026 metrics, assume monthly revenue is $52,560. The marketing budget, set at 30% of revenue, is $15,768. If that spend resulted in 100 new patients signing up, the PAC calculation looks like this:
PAC = $15,768 / 100 New Patients = $157.68 per patient
Tips and Trics
Track marketing spend by channel, not just total dollars spent.
Isolate marketing costs from general administrative overhead expenses.
If PAC rises while new patient volume is flat, marketing channels are saturated.
Ensure you account for the 50% Billing & Collections Fees when assessing true net revenue from new patients.
KPI 5
: Operating Expense Ratio (OER)
Definition
Turning the Year 1 EBITDA loss of $61,000 into a $341,000 profit in Year 2 absolutely requires the Operating Expense Ratio (OER) to drop significantly. This ratio measures how much revenue is eaten up by overhead, making it the key lever for achieving profitability in this high-fixed-cost clinic model. A lower OER means you are running a tighter ship relative to the revenue you generate.
Advantages
Directly links overhead control to bottom-line EBITDA results.
Highlights the impact of scaling fixed costs like the $12,000 monthly rent.
Forces management to focus on revenue density per provider.
Disadvantages
Can hide poor gross margin performance if COGS are ignored.
A ratio that drops too fast might signal under-investment in patient acquisition.
It’s less useful if revenue is highly volatile or unpredictable.
Industry Benchmarks
For primary care models relying on fee-for-service revenue and carrying significant fixed overhead, the OER needs to be aggressively managed. While some high-volume clinics might tolerate OERs near 50%, to cover high fixed costs and generate profit, you defintely need to push this ratio down toward 35% or lower as you scale. This ratio is critical because it shows if your volume growth is actually covering your rent and administrative salaries.
How To Improve
Increase Provider Utilization Rate to spread fixed costs over more treatments.
Focus on improving Revenue Per Visit (RPV) through better service mix.
Lock in favorable, long-term rates for fixed overhead components like rent.
How To Calculate
The Operating Expense Ratio is found by taking all expenses not directly tied to delivering the service (like rent, salaries, utilities, marketing) and dividing that sum by your total revenue. This calculation tells you the percentage of sales consumed by operations.
OER = Total Operating Expenses / Total Revenue
Example of Calculation
To move from a $61,000 loss to a $341,000 profit, the clinic needs an operating income swing of $402,000 between Year 1 and Year 2. If we assume Year 1 Revenue was $1,500,000, the Year 1 OER must have been high enough to absorb that loss. The required drop in the ratio is calculated by dividing the required swing by the revenue base.
Required OER Drop = $402,000 / $1,500,000 = 0.268 or 26.8 percentage points
If Year 1 OER was 75%, Year 2 OER must be approximately 48.2% to achieve the target profit, assuming revenue and COGS remained stable, which shows the massive operational efficiency needed.
Tips and Trics
Separate fixed OpEx (like $12,000 rent) from variable OpEx immediately.
Track OER monthly, not just quarterly, to catch cost creep early.
Benchmark your OER against the required 850% Provider Utilization Rate goal.
If Billing & Collections Fees (50% of revenue cycle cost) are included in OpEx, focus on improving the Working Capital Cycle.
KPI 6
: Months to Breakeven
Definition
Months to Breakeven is the time it takes for your total accumulated earnings to equal your total accumulated expenses since you started operating. This metric shows when the business stops burning cash from its initial investment. For this clinic, hitting this milestone by January 2027, or 13 months from launch, is critical to managing cash risk.
Advantages
Provides a hard deadline for achieving operational self-sufficiency.
Directly informs runway planning and future capital needs.
Forces management to focus on margin improvement immediately.
Disadvantages
It is backward-looking, based on past performance, not future projections.
It can mask poor cash flow if collections lag significantly behind revenue recognition.
It doesn't account for the cost of capital used to fund the initial losses.
Industry Benchmarks
For specialized service providers like clinics, a 12 to 18 month breakeven timeline is common, especially when fixed overhead is high, like the $12,000 monthly rent here. If you are heavily reliant on slow insurance reimbursements, this period can easily stretch past two years.
How To Improve
Immediately push Gross Margin Percentage toward the 90%+ target.
Increase service volume by driving Provider Utilization Rate above the starting 600%.
Optimize scheduling to maximize Revenue Per Visit (RPV) above the $131 average.
How To Calculate
To find the time to breakeven, you divide the total cumulative fixed costs incurred up to the start of the measurement period by the average monthly contribution margin achieved during the period. This calculation shows how many months of positive contribution are needed to erase the initial deficit.
Months to Breakeven = Total Cumulative Fixed Costs / Average Monthly Contribution Margin
Example of Calculation
The clinic recorded a $61,000 EBITDA loss in Year 1, representing the initial cumulative loss that must be recovered. If the clinic can achieve a consistent monthly contribution margin of $15,000 starting in month 13, the time needed to recover just the Year 1 loss would be 4.07 months. However, since the goal is to hit breakeven by month 13, the cumulative contribution over those 13 months must cover all fixed costs incurred during that time.
Track cumulative cash burn monthly to see if you are on track for the January 2027 deadline.
Model the impact of the 50% Billing & Collections Fees on actual cash realization versus reported revenue.
If Operating Expense Ratio (OER) doesn't drop sharply from Year 1 to Year 2, breakeven will slip.
It is defintely crucial to monitor utilization rates; if they lag the 600% start, profitability suffers immediately.
KPI 7
: Working Capital Cycle
Definition
The Working Capital Cycle (WCC) measures how long your cash is tied up in operations before it cycles back as collected revenue. For this clinic, it specifically tracks the delay between delivering care and receiving payment from insurance carriers. A long cycle means you fund operations—like paying staff before reimbursement—for longer periods.
Advantages
Pinpoints cash flow strain caused by slow insurance reimbursement timelines.
Helps manage the impact of the 50% Billing & Collections Fees by prioritizing fast cash conversion.
Informs decisions on short-term credit needs to bridge the gap between service and payment.
Disadvantages
It doesn't directly measure profitability, only liquidity timing.
A short cycle can mask underlying issues if the Revenue Per Visit is too low.
It's heavily influenced by external factors, namely insurance company payment speeds.
Industry Benchmarks
In general healthcare, Days Sales Outstanding (DSO), the main driver of the WCC, should ideally be under 45 days. However, because your model relies on third-party payers and incurs a high 50% fee on collections, your target DSO must be significantly lower than the industry average to maintain adequate cash flow.
How To Improve
Streamline claim scrubbing and submission to happen within 24 hours of service delivery.
Aggressively pursue faster payment contracts with major insurance carriers.
Focus practitioner scheduling to maximize visits with high-reimbursement payers first.
How To Calculate
The cycle is calculated by adding the time inventory sits before use (Days Inventory Outstanding, DIO) to the time it takes to collect payment (Days Sales Outstanding, DSO), then subtracting how long you take to pay vendors (Days Payables Outstanding, DPO). For a service business, DIO is usually minimal.
Example of Calculation
Let's look at the cash conversion lag. If you deliver care today, bu
The most critical metric is Provider Utilization Rate, as low utilization (like 600% for 2026 GPs) directly causes the initial $61,000 EBITDA loss, delaying breakeven past 12 months
Fixed costs total $20,100 monthly (including $12,000 rent and $1,800 EHR software); these must be absorbed quickly by increasing patient volume and RPV
Expand support staff (eg, Medical Assistants from 20 FTE to 30 FTE in 2027) only when provider utilization rates justify the added wage expense
About the author
Paul Wells
Practical Finance Writer
Paul Wells is a practical finance writer for Financial Models Lab who focuses on cost-to-open estimates and monthly expense breakdowns that help founders avoid common launch mistakes. He simplifies business plans for non-finance readers and brings a grounded, founder-minded perspective to startup cost research.
Choosing a selection results in a full page refresh.