Primary Care Clinic Startup Costs: $345K CAPEX And $558K Cash
It costs enough to fund the clinic through buildout, launch, and the early reimbursement ramp, with the model showing a $558K minimum cash need and $345K of CAPEX CAPEX, meaning long-lived assets, includes $150K for clinic renovation, $75K for medical diagnostic equipment, $40K for exam room furnishings, $30K for IT setup, and other launch assets Pre-opening expenses include licensing, credentialing, insurance binders, legal review, accounting setup, training, and launch readiness, but those items are not separately priced in the provided model Working capital is the real safety net: fixed overhead starts at $201K per month, support payroll is $3025K in Year 1, and breakeven is not modeled until Month 13
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a primary care clinic, then adds a contingency reserve.
!
CAPEX only Base CAPEX is $345,000 across Month 1 to Month 6 before contingency. This excludes working capital, payroll runway, debt service, deposits, licensing fees, marketing, operating losses, and inventory runway.
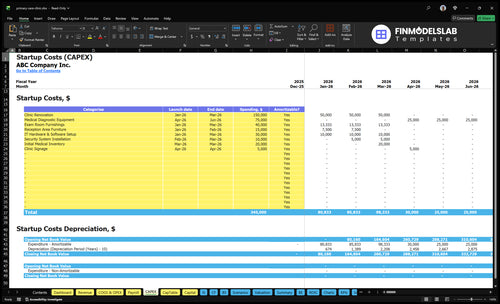
What does the Primary Care Clinic startup cost screenshot show?
This screenshot shows the CAPEX tab in the Primary Care Clinic Financial Model Template, with startup expenses, launch timing, and depreciation or amortization logic. It should also show $345K CAPEX, $558K minimum cash, Month 13 breakeven, and Year 1 EBITDA of -$61K and Year 2 EBITDA of $341K; review the assumptions.
Key screenshot highlights
Startup cost categories
Cash and payback timing
Hiring and revenue ramp
Primary Care Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What drives primary care clinic buildout and equipment cost?
For a Primary Care Clinic, the buildout and equipment budget starts around $300K: $150K renovation, $75K diagnostic equipment, $40K exam room furnishings, $15K reception furniture, $10K security, and $5K signage. Here’s the quick math: that spend covers the clinic spaces and core flow, not just the visible furniture. Lease condition and landlord allowance can move the final cash need.
Buildout cost
$150K clinic renovation
Reception and waiting area flow
Restrooms, flooring, lighting
Plumbing, electrical, accessibility-ready layout
Room readiness
$75K medical diagnostic equipment
$40K exam room furnishings
Lab area and vaccine storage
ECG, scales, exam tables, supplies
How much working capital is needed for a primary care clinic?
For a Primary Care Clinic, treat working capital separately from CAPEX and pre-opening spend: the core plan is a $558K minimum cash need and Month 13 breakeven. For owner context, see How Much Does The Owner Make From A Primary Care Clinic? Monthly fixed overhead is $201K, and Year 1 support payroll is $3,025K before provider compensation assumptions, so cash gets tight fast.
Cash plan
$558K minimum cash need
Month 13 breakeven target
$201K monthly fixed overhead
$3,025K Year 1 support payroll
Cash gaps
50% billing and collections fees
35% medical supplies
45% lab and diagnostic fees
30% patient acquisition marketing
Payer credentialing and reimbursement lag are the big cash-gap risks. If claims slow down, the clinic still pays overhead now and collects later.
How do you fund a primary care clinic startup?
For a Primary Care Clinic, fund the build for $345K in CAPEX plus at least $558K in cash, because the model does not break even until Month 13 and only pays back in 29 months. Use a Year 1 plan with 2 GPs, 1 nurse practitioner, and 1 physician assistant, with modeled prices of $150 for GP visits and $120 for NP and PA visits. That plan only works if you stress-test credentialing delays, slower patient volume, billing collections, staffing start dates, and lease timing before you raise capital.
Funding base
$345K CAPEX to open.
$558K minimum cash need.
Month 13 breakeven.
29-month payback.
Year 1 stress test
2 GPs, 1 NP, 1 PA.
$150 GP visit price.
$120 NP and PA visit price.
Test 600% and 550% capacity.
Calculate Fuding Needs
Startup cost summary
Startup costs cover build-out, medical equipment, furnishings, IT setup, and launch cash before Month 13 breakeven.
Highlighted CAPEX$345,000Base planning example
Excluded cash needs$558,000Outside CAPEX total
Funding need$903,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinic Renovation and Leasehold Improvements
$150,000
Build-out scope and contractor pricing
Yes
Medical Diagnostic Equipment
$75,000
Equipment mix and vendor quotes
Yes
Exam Room Furnishings and Reception Furniture
$55,000
Room count, finish level, and furniture specs
Yes
IT Hardware and Software Setup
$30,000
Hardware count, EHR setup, and installation scope
Yes
Initial Medical Inventory, Security, and Signage
$35,000
Opening stock, security install, and site signage
Yes
Operating Reserve Through Breakeven
$558,000
Launch losses and fixed overhead before Month 13 breakeven
No
Primary Care Clinic Core Five Startup Costs
Leasehold Improvements Startup Expense
Buildout Scope
Classify the clinic buildout as CAPEX when it creates permanent value. The source budget is $150K from Month 1 to Month 3 for reception, waiting area, exam rooms, nurse station, restrooms, flooring, lighting, plumbing, electrical, accessibility-ready layout, security tie-ins, and signage.
Cost Inputs
Estimate this cost from the lease condition, square footage, exam room count, plumbing changes, electrical capacity, landlord allowance, permitting, and whether the prior use was medical. Here’s the quick math: buildout pricing usually starts with contractor quotes plus tenant work scope, then adds separate $5K signage and $10K security installation if they are included in CAPEX.
Keep It Lean
Cut this cost by reusing a prior medical layout, limiting plumbing moves, and matching the floor plan to the fewest exam rooms that still support demand. The big mistake is paying for cosmetic upgrades before code and layout needs are set. A clean landlord allowance can shrink the cash hit, but only if the lease terms are clear up front.
CAPEX Timing
Book renovation spend when invoices tie to permanent improvements, not routine repairs. For a primary care clinic, that means tracking the buildout in the opening budget and keeping separate lines for the $5K signage and $10K security install so fixed assets, depreciation, and opening cash needs stay clean.
Medical Equipment And Exam Room Setup Startup Expense
Setup Budget
Plan three buys: $40K for exam room furnishings in Months 1 to 3, $20K for initial medical inventory in Month 3, and $75K for medical diagnostic equipment in Months 4 to 6. That covers exam tables, diagnostic sets, scales, ECG, refrigeration, vaccine storage, procedure supplies, lab gear, and an autoclave only if the service mix needs it.
What To Include
Estimate each line by unit count, quotes, and install timing. Keep durable equipment separate from consumable supplies, because ongoing medical supplies are modeled at 35% of Year 1 revenue and lab and diagnostic fees at 45%. That split keeps startup cash from being padded with operating spend.
Control Spend
Trim cost by buying only the devices your service mix needs, and skip an autoclave unless you truly need in-house sterilization. Get at least two vendor quotes, phase purchases with opening dates, and avoid overbuying inventory before patient flow is proven. The big risk is mixing one-time setup with recurring supply burn.
Stage The Buy
Match spending to the rollout: furnishings first, inventory in Month 3, diagnostics in Months 4 to 6. That staging protects cash and lets you confirm room count, plumbing, electrical load, and service demand before the larger equipment buy lands.
EHR, IT, Communications, And Billing Setup Startup Expense
Setup CAPEX
Use $30K as CAPEX for Month 1 to 3 IT and communications setup. It covers EHR onboarding, practice management, billing setup, computers, networking, cybersecurity, patient portal, phones, printers, telehealth tools, and access controls. Keep this separate from recurring software and service fees.
How To Estimate
Estimate it from vendor quotes, device count, and install time. Add one-time hardware, implementation, and go-live work only. The recurring $18K per month EHR fee is an operating cost, not CAPEX. Billing and collections are modeled at 50% of Year 1 revenue, so cash needs rise fast as volume grows.
Control The Run Rate
The safest savings come from right-sizing devices, using fewer user licenses at launch, and staging noncritical tools after go-live. Do not bury support, subscriptions, or billing fees inside startup assets. One clean line: separate build cost from monthly run cost, or your burn rate will look too low.
Cash Timing
For a primary care clinic, the real risk is timing: a one-time setup budget can be finished in Month 3, but the $18K monthly EHR bill and 50% billing and collections fee keep hitting cash every month after launch.
Licensing, Credentialing, Insurance, And Professional Fees Startup Expense
Regulated setup
Put licensing, credentialing, insurance, and professional fees in pre-opening or early operating costs, not equipment. In this model, insurance runs at $25K per month and professional services at $800 per month for formation, payer enrollment, malpractice, general liability, and compliance work. That cost can start before the first visit.
What it covers
This bucket covers entity formation, state medical business rules, provider credentialing, payer enrollment, CLIA waiver if needed, legal review, accounting setup, and compliance policies. Use months of coverage × monthly cost to budget it, plus quotes by state and provider type. Costs vary with payer mix and service scope.
Monthly insurance: $25K
Professional services: $800
State and payer rules drive variance
How to budget it
Start with written quotes, then add enough months to cover slow approvals. Credentialing delays can push cash needs past the equipment budget, so build runway for pre-opening time too. Keep legal advice separate from finance assumptions. One clean rule: if revenue cannot start, this cost still runs.
Get insurer and counsel quotes
Model delay months, not best case
Separate this from equipment CAPEX
Runway risk
If credentialing slips, the clinic may burn cash for longer before billing starts. That makes this line item a cash runway issue, not just a compliance task. Watch the gap between opening date, first payer approval, and first reimbursable visit; that gap is what usually surprises founders.
Staffing Readiness, Launch Payroll, And Working Capital Startup Expense
Launch Payroll
Keep pre-opening payroll and working capital out of CAPEX. For Year 1 support staff, the model totals $3.025M before taxes and benefits: clinic managers, front desk, billers, medical assistants, IT support, and HR admin. Provider pay is not supplied, so model that line separately.
Support Payroll
Here’s the quick math: 10 clinic managers at $85K, 10 front desk coordinators at $40K, 10 medical billers at $55K, 20 medical assistants at $35K, 5 IT support specialists at $60K, and 5 HR admins at $45K. That equals $3.025M annual support payroll.
Use headcount times salary.
Add taxes and benefits separately.
Model provider pay on its own.
Runway Need
Working capital must fund payroll, rent, insurance, utilities, supplies, billing, and reimbursement delays until Month 13 breakeven. The key input is months of coverage, then multiply by monthly operating burn. If onboarding or payer enrollment slips, cash needs rise fast because revenue lags while staff and overhead start first.
Budget for the full gap period.
Track reimbursement timing weekly.
Keep a cash buffer for delays.
Cash Bridge
Set the launch cash bridge from the opening date through Month 13, not just the buildout period. That bridge should cover staff pay, fixed clinic costs, and slow collections, while CAPEX stays limited to buildout and equipment. If the clinic opens before payer billing is stable, cash needs move up even when the space is ready.
Compare 3 Startup Cost Scenarios
Startup cost scenarios
Startup cost moves fast with clinic size because buildout, equipment, staffing, and working capital all scale together. Lean, base, and full show the cash gap between a solo launch and a larger multi-provider practice.
Lean, base, and full clinic launch funding needs.
Scenario
Lean LaunchSolo provider launch
Base LaunchStandard independent practice
Full LaunchLarger multi-provider clinic
Launch model
Solo provider launch with reduced room count, lighter equipment, and tighter working capital.
Standard independent practice with 2 GPs, 1 nurse practitioner, and 1 physician assistant, using $345K CAPEX and $558K minimum cash.
Larger multi-provider launch with more rooms, deeper equipment, and more runway.
Typical setup
It starts small and keeps the buildout and staffing focused on one provider schedule.
It follows the modeled clinic setup with $201K monthly fixed overhead and Month 13 breakeven.
It pushes the footprint wider so more providers can open at once and absorb slower ramp-up.
Cost drivers
Smaller buildout
fewer exam rooms
lighter equipment
lower payroll
less working capital
Clinic renovation
medical equipment
provider payroll
rent and utilities
working capital
Larger buildout
more exam rooms
deeper equipment
added provider payroll
more runway
Planning rangeCAPEX only
Below base-case fundingLower cash need
Modeled base-case fundingBaseline plan
Above base-case fundingHigher cash need
Best fit
Best for founders who want to test demand before adding more providers.
Best for an operator who wants the sourced model as the launch target.
Best for teams that want a bigger footprint from day one.
!
Planning note: These ranges are researched planning assumptions from the model, not exact vendor or contractor quotes. Replace them with local pricing, staffing quotes, and lease terms before you fund the launch.
Plan around the model’s $558K minimum cash need, not just the $345K CAPEX list That cash must carry the clinic through renovation, equipment setup, hiring, and collections ramp The fixed overhead alone is $201K per month, before the $3025K Year 1 support payroll and any provider compensation assumptions not supplied
The model reaches breakeven in Month 13 That matters because Year 1 EBITDA is still negative at -$61K, while Year 2 EBITDA rises to $341K Payback is modeled at 29 months, so the opening plan needs enough runway for more than the first few billing cycles
Yes, credentialing should start before opening because payer enrollment can delay collections even when the clinic is ready to see patients The Year 1 care team includes 2 GPs, 1 nurse practitioner, and 1 physician assistant If credentialing lags, the clinic still carries $12K rent, $25K insurance, and payroll costs
Choose the lease around the launch staffing plan, not a generic medical office size The base model starts with 2 GPs, 1 nurse practitioner, 1 physician assistant, 2 medical assistants, front desk, billing, and management The renovation budget is $150K, so extra square footage can quickly turn into unused CAPEX and higher rent
The clinic keeps paying fixed overhead and volume-based costs after launch Fixed overhead is $201K per month, including $12K rent, $18K EHR fees, and $25K insurance Variable costs include 50% billing and collections fees, 35% medical supplies, 45% lab and diagnostic fees, and 30% patient acquisition marketing in Year 1
About the author
Samuel Price
Launch Planning Specialist
Samuel Price is a launch planning specialist at Financial Models Lab who helps side-hustle builders test whether a business idea is financially realistic. He turns business questions into clear planning steps, with a focus on operating cost estimates for opening and running small businesses. His research-based writing highlights the common costs new founders often miss.
Choosing a selection results in a full page refresh.