Peptide Therapy Clinic Strategies to Increase Profitability
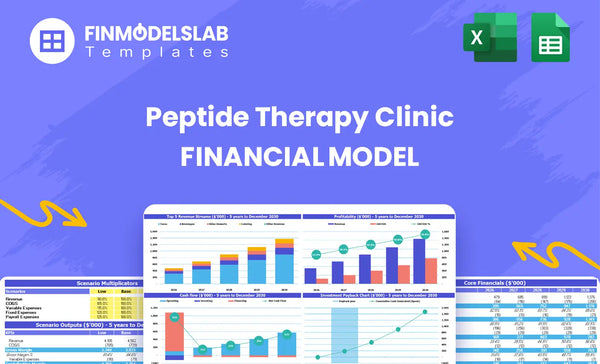
Your Peptide Therapy Clinic starts with a strong margin profile, targeting an initial EBITDA margin of around 340% in 2026 The goal is to scale this toward 55% or higher within three years by optimizing staff utilization and reducing supply chain costs Initial annualized revenue is projected near $147 million, but the high fixed costs-including $20,000 monthly for facility and operations, plus administrative wages-demand high patient volume
7 Strategies to Increase Profitability of Peptide Therapy Clinic
#
Strategy
Profit Lever
Description
Expected Impact
1
Maximize Staff Utilization
Productivity
Fill the 45% RN capacity gap and 55% Health Coach gap starting in 2026.
Drives high contribution margin since fixed costs are already covered.
2
Implement Tiered Pricing
Pricing
Raise MD treatment prices from $850 in 2026 to $950 by 2030 and introduce premium packages.
Achieves 3-5% annual price increase across key services.
Directly increases the overall Average Transaction Value (ATV).
4
Negotiate Peptide Sourcing
COGS
Consolidate vendors to force a 10-15% cost reduction on Sourcing (85% of revenue) and Lab Fees (45% of revenue).
Significantly lowers variable costs tied to service delivery.
5
Right-Size Clinical Labor
Productivity
Make sure high-cost MDs focus only on complex cases, delegating routine tasks to RNs or Phlebotomists.
Improves utilization rate for $850 per treatment staff time.
6
Lower Customer Acquisition Cost (CAC)
OPEX
Reduce Digital Marketing spend from 60% of revenue down to 40% by Year 4 by prioritizing retention.
Cuts the high initial cash burn associated with new patient acquisition.
7
Review Overhead Leases
OPEX
Scrutinize the $12,500/month Premium Clinic Lease and other non-wage fixed overhead upon renewal dates.
Reduces the $20,000 monthly fixed overhead burden.
Peptide Therapy Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What is our true contribution margin (CM) per treatment type right now?
Determining your true contribution margin (CM) requires subtracting all variable costs-peptides, lab fees, supplies, and acquisition costs-from the service price for MD, NP, and RN offerings to pinpoint which mix drives the highest dollar contribution, a key step detailed in How To Write A Business Plan For Peptide Therapy Clinic? If the average MD service price is $1,200 with variable costs totaling $500, the CM is $700; you need to map this against the volume you can actually handle. Honestly, focusing only on the highest percentage margin service can hide lower absolute dollar returns.
Variable Cost Breakdown
Isolate the cost of the specific peptide compound per dose.
Track lab fees associated with biomarker testing.
Calculate the cost of supplies, like syringes and vials.
Allocate patient acquisition costs (CAC) to each service type.
Define what portion of practitioner time is truly variable.
Contribution Drivers
MD service yields the highest dollar CM, say $700 per treatment.
NP service might offer a better percentage margin, maybe 56%.
Focus volume on the service with the highest absolute dollar contribution.
If RN treatments are only $200 CM, ensure they fill scheduling gaps, not primary slots.
We need to defintely track the mix shift month-over-month.
How quickly can we push clinical staff utilization rates above 70%?
Reaching 70% utilization for your Peptide Therapy Clinic staff requires immediate, targeted patient acquisition growth, as current 2026 projections sit significantly lower at 55% for MDs and 45% for RNs, a scenario we explore defintely when looking at What Are Peptide Therapy Clinic Operating Costs?. We must tightly link marketing spend, currently 60% of revenue, to patient volume to ensure the Patient Acquisition Cost (PAC) remains healthy against Lifetime Value (LTV).
Marketing currently consumes 60% of total revenue.
You must lift patient volume without letting marketing costs grow faster than revenue.
Fixed overhead coverage depends entirely on filling these provider schedules.
Mapping Acquisition Costs
Calculate the maximum allowable PAC based on average LTV.
If acquisition is too expensive, utilization gains won't translate to profit.
Focus on protocols that drive high retention to increase LTV.
If PAC exceeds one-third of LTV, you're overpaying for growth.
Where are we losing time or money due to clinical workflow inefficiencies?
Workflow inefficiencies in your Peptide Therapy Clinic are defintely costing you money by slowing patient throughput and forcing expensive Registered Nurses (RNs) to handle tasks lower-cost staff should manage. We need to map the patient journey right now to find where time bleeds out, especially around diagnostics and scheduling; you can see a deeper dive into related expenses here: What Are Peptide Therapy Clinic Operating Costs?
Pinpointing Labor Leakage
Stop RNs from doing administrative scheduling tasks immediately.
Calculate the direct cost of task mismatch per hour.
If an RN spends 10 hours weekly coordinating, that's $500 lost value weekly.
Audit EMR use; slow systems add minutes to every patient touchpoint.
Fixing Diagnostic Flow
Phlebotomy utilization is only 60%; this is a major bottleneck.
Map the exact time from patient check-in to blood draw completion.
If a Patient Coordinator can prep vials, free up the RN for clinical review.
Analyze if follow-up scheduling requires physician sign-off every time.
Are we willing to raise prices or bundle services to capture more value?
Yes, you should defintely test a modest price increase on physician services immediately to gauge market tolerance while simultaneously pushing volume toward higher-margin NP services. Understanding the financial impact of these changes is crucial, which is why you need to review What Are Peptide Therapy Clinic Operating Costs? before making final decisions.
Test MD Pricing Power
Test a 5% price increase on high-demand MD services.
MD services currently start at $850.
Measure ARPP gain against patient churn risk.
If churn stays below 3%, the test is a win.
Optimize Service Mix
Shift practitioner capacity to Nurse Practitioner (NP) services.
NP services should carry a higher contribution margin.
Bundle initial MD consults with subsequent NP visits.
Value capture comes from efficient practitioner utilization.
Peptide Therapy Clinic Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Key Takeaways
Achieving target profitability hinges on immediately pushing clinical staff utilization rates above 70% to maximize revenue from existing fixed cost structures.
The most immediate profit boost comes from aggressively negotiating peptide sourcing and lab fees to reduce the Cost of Goods Sold (COGS) percentage.
Sustainable margin growth requires actively shifting the patient service mix toward higher-margin NP treatments and implementing modest annual price increases.
Workflow optimization and rigorously right-sizing labor ensure that high-cost providers are reserved exclusively for the highest-value patient interactions.
Strategy 1
: Maximize Staff Utilization
Focus on Utilization
You need to aggressively fill the 45% RN gap and 55% Health Coach gap projected for 2026. Since fixed overhead is already covered by existing volume, every new treatment booked through these underutilized roles drops almost entirely to the bottom line as pure contribution margin. This is where immediate profit lives.
Cost of Unused Time
Unfilled capacity is a hidden fixed cost. If RN salaries are $120,000 annually, a 45% gap means you are losing $54,000 in potential revenue generation per RN before accounting for variable costs. This calculation requires knowing total staff payroll against maximum potential treatment volume. What this estimate hides is the opportunity cost of delayed patient care.
RN Annual Salary: $120,000
Target RN Treatment Price: $250
Lost Revenue Potential: 45% of total RN capacity value.
Filling the Capacity
To capture this margin, push patients toward RN services priced at $250, rather than only high-end Medical Doctor consultations. Shift routine follow-ups away from $850 MDs to fill RN schedules first. Health Coaches need specific marketing pushes to fill their 55% void, perhaps bundling initial assessments. Defintely focus on scheduling efficiency.
Prioritize RN bookings ($250 ATV).
Delegate routine tasks from MDs.
Create specific Health Coach intake packages.
Immediate Profit Lever
Once fixed overhead is covered-say, by existing MD revenue-every $250 RN treatment generates near-full contribution margin, assuming variable costs like peptides are manageable. This means aggressive scheduling incentives for RNs and Coaches now directly translate to immediate, high-quality profit growth, bypassing the need for major new overhead spending.
Strategy 2
: Implement Tiered Pricing
Anchor Price Increases
You need systematic price increases coupled with value bundling to lift revenue per patient. Plan to raise average treatment prices by 3-5% yearly. Introduce premium packages that lock in high-value services like coaching and diagnostics right at the start.
Calculate Price Velocity
Calculate the required annual growth rate to hit the target price points. For MD services, moving from $850 in 2026 to $950 by 2030 requires a compound annual growth rate of about 2.8%. Premium tiers must bundle high-cost inputs like biomarker analysis and coaching to justify the higher price point immediately.
Current service prices
Target price escalator (3-5%)
Cost of bundled diagnostics
Bundle for Higher ATV
Don't just raise the base price; structure packages that force adoption of higher-value services. Premium tiers should automatically include initial coaching sessions and comprehensive diagnostics. This immediately lifts the Average Transaction Value (ATV) and covers upfront service costs before subsequent monthly treatments begin.
Mandate diagnostics in top tier
Price coaching sessions into packages
Ensure MDs only bill premium rates
Justify Every Increase
Affluent clients expect measurable ROI for every dollar spent on longevity treatments. If your 3-5% annual escalator isn't clearly tied to improved biomarker results or enhanced coaching access, patient churn risk increases defintely. Stick to the plan, but justify the increase every time.
Strategy 3
: Optimize Service Mix
Shift Service Focus
You must steer volume from Registered Nurse (RN) services priced at $250 to Nurse Practitioner (NP) treatments priced at $450. This direct service mix optimization immediately lifts your Average Transaction Value (ATV). If 50% of volume shifts from RN to NP, your blended ATV jumps from $350 to $400, assuming equal volume distribution across both tiers.
Pricing Inputs Needed
Service mix is driven by practitioner time allocation and protocol complexity. To model this, you need the exact fee structure for every service tier: the $450 NP rate versus the $250 RN rate. This calculation determines your true revenue per hour of clinical capacity, which is crucial since revenue depends on practitioner output, not just patient count.
Driving High-Margin Sales
To execute this shift, train front-office staff to present the higher-value NP option first. Structure incentives for practitioners to recommend the $450 protocol over the $250 one. You want the patient journey to defintely favor the higher contribution service, maximizing revenue per available appointment slot.
Watch the Mix Ratio
Track the percentage split between $450 NP services and $250 RN services weekly. If the ratio drifts toward RN services, overall margin erodes quickly, even if volume stays high. You need tight operational oversight here to maintain target profitability.
Strategy 4
: Negotiate Peptide Sourcing
Target COGS Reduction
You must aggressively target cost of goods sold (COGS) components now, specifically sourcing and lab work. Aim to cut Compounded Peptide Sourcing, which is currently 85% of revenue, by 10-15%. Simultaneously, reduce Diagnostic Laboratory Fees, starting at 45% of revenue, by the same margin. This directly impacts gross margin quickly.
Cost Inputs
Peptide Sourcing covers the active ingredients needed for treatment protocols. Lab fees cover the biomarker analysis required for personalized dosing. To model savings, you need current vendor quotes and projected annual volume commitments. These two costs alone represent 130% of your current revenue base. What this estimate hides is that these are variable costs tied directly to service delivery.
Peptide cost: 85% revenue share.
Lab fees: 45% revenue share.
Total variable cost pressure.
Vendor Leverage
Reducing these high variable costs requires leverage. Stop using multiple small suppliers for peptides; consolidate purchasing power with one or two primary sources. Offer them guaranteed minimum annual spend for a steep discount. For labs, commit to a higher volume tier for testing to secure better per-test pricing. This is defintely doable.
Consolidate peptide vendors now.
Commit to higher annual volume.
Negotiate better tier pricing.
Margin Impact
If you achieve the low end of the target, a 10% reduction on the 85% sourcing cost frees up 8.5% of revenue. If you hit 15% on the 45% lab fees, that's another 6.75%. That combined 15.25% margin improvement flows straight to the bottom line, assuming fixed costs remain static.
Strategy 5
: Right-Size Clinical Labor
Align Labor Value
You must immediately separate high-value Medical Doctor work from routine tasks. An MD consultation brings in $850, but Registered Nurse time costs significantly less. Shifting simple follow-ups to RNs or Phlebotomists protects your highest-margin labor for complex cases. That's how you improve unit economics fast.
MD Cost Input
Clinical labor cost is driven by the price per service slot, not just salary. The $850 MD treatment price is a direct input into your revenue calculation. You need hours billed versus revenue generated by role to see true utilization. What this estimate hides is the opportunity cost of using an MD for a $250 RN task.
MD Price: $850 per treatment
RN Price: $250 per service
Focus: High-value MD time
Delegation Tactics
Stop using your most expensive asset for low-leverage work. If an RN can handle the initial intake or blood draw (Phlebotomist work), the MD only steps in for complex protocol adjustments. This delegation protects the $850 revenue stream and maximizes output per physician hour. Don't defintely overpay for routine care.
Shift intake tasks now
Protect MD $850 slots
Use RNs for $250 services
Utilization Lever
Every routine task delegated from an MD to an RN or Phlebotomist frees up capacity that generates $600 more margin per slot ($850 minus $250). This is a direct, measurable increase to contribution margin without raising prices or finding new patients.
You've got to aggressively shift acquisition spend away from digital channels. Moving Customer Acquisition Cost (CAC) from 60% of revenue down to 40% by Year 4 requires prioritizing patient retention and referral programs over costly new patient buys. This shift is crucial for margin expansion, defintely.
Initial Acquisition Drag
The initial 60% of revenue dedicated to acquisition reflects the high cost of reaching affluent clients seeking specialized peptide therapy. To calculate this, you need total monthly spend on digital ads, SEO, and lead generation against total monthly revenue. If initial revenue is $100k, $60k goes to CAC. This is unsustainable long-term.
Monthly digital ad spend.
Cost per qualified lead (CPQL).
New patient conversion rate.
Lowering Acquisition Drag
Achieving the 40% CAC target means investing in programs that drive organic growth. Referrals and keeping existing patients are cheaper than constantly buying new ones. If a new patient costs $1,500 to acquire digitally, a referral might cost $150 in incentives. You must track patient lifetime value (LTV) versus CAC closely.
Launch a tiered patient referral bonus.
Increase patient engagement touchpoints.
Focus on high-value patient retention rates.
Retention Profit Lift
Every percentage point you shave off CAC directly flows to contribution margin, especially since fixed costs are covered by existing utilization. If you save 20% of revenue ($20k on $100k revenue) by Year 4, that $20k is pure profit lift, assuming variable costs remain stable. This is a massive lever for profitability.
Strategy 7
: Review Overhead Leases
Cut Fixed Lease Costs
Your fixed overhead, excluding wages, sits at $20,000 monthly, which pressures profitability immediately. The Premium Clinic Lease at $12,500 is the single biggest lever here. You must aggressively negotiate this cost when the lease comes up for renewal to improve your runway.
Pinpoint Overhead Spend
This $20,000 monthly fixed spend covers essential non-wage overhead. The primary input is the $12,500 lease payment for your physical clinic space. Insurance costs are also bundled here. If you hit break-even at $20k fixed, every dollar saved directly boosts net income, so this cost needs immediate attention.
Negotiate Lease Timing
Focus negotiation efforts on the lease renewal date, which is your best leverage point. Look at comparable market rates for similar square footage in your metro area. If you achieve even a 10% reduction on the lease, that's $1,250 saved monthly, or $15,000 annually. Don't forget to shop insurance quotes too.
Action on Lease Expiration
Track the exact date your Premium Clinic Lease expires; this dictates when you can push for better terms. If market rents have flattened or dropped, aim to cut that $12,500 line item by at least 5%. Defintely review all insurance policies against competitors' coverage levels before renewing.
A stable clinic should aim for an EBITDA margin between 45% and 60%, significantly higher than the initial 340% projected margin, by scaling revenue past $25 million annually (Year 2)
The model shows a break-even date in January 2026, with a rapid payback period of 13 months, assuming the initial $400,500 capital expenditure is funded
Focus on reducing the 13% COGS (peptides and lab fees) first, as cutting fixed costs like the $12,500 monthly lease is harder
Yes, planned price increases (eg, MD treatment rising from $850 to $950 by 2030) are essential to outpace inflation and maintain margin integrity
Choosing a selection results in a full page refresh.