Dermal Filler Injection Training Startup Costs: $791k Cash Need
Plan for $1605k in upfront CAPEX to open a dermal filler training business, before working capital and early operating runway Total funding need is much higher because payroll, rent, insurance, compliance, marketing, and injectable supplies start in Month 1 the model shows a $791k minimum cash requirement in Month 2 These are researched planning assumptions, not vendor quotes or guaranteed pricing In Year 1, the model assumes 12 billable days per month, 65% occupancy, and course pricing from $3,200 to $8,500
Calculate Fuding Needs
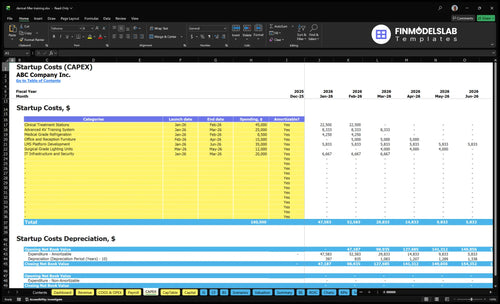
Startup cost summary
This table separates startup CAPEX from the non-CAPEX cash reserve needed to launch and reach early breakeven.
Highlighted CAPEX$140,000Base planning example
Excluded cash needs$791,000Outside CAPEX total
Funding need$931,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinical Treatment Stations
$45,000
Training room buildout and treatment station count
Yes
LMS Platform Development
$35,000
Course delivery setup and content build scope
Yes
Advanced AV Training System
$25,000
Video capture, display, and demo equipment
Yes
IT Infrastructure and Security
$20,000
Network, devices, and data protection setup
Yes
Office and Reception Furniture
$15,000
Front-of-house furnishing and admin workspace fit-out
Yes
Operating Cash Reserve
$791,000
Month 2 cash trough, payroll runway, and launch burn
No
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets for a dermal filler injection training launch, not operating cash or runway.
!
CAPEX only Excludes inventory, payroll runway, deposits, debt service, working capital, marketing, insurance premiums, rent runway, and disposable supply replenishment unless those items are capitalized.
What does the Dermal Filler Injection Training screenshot show?
Lean cuts CAPEX and rent, Base matches the model at about $160.5k CAPEX and $21.45k monthly fixed costs, and Full adds rooms, staff, and working capital.
Lean, Base, and Full startup cost comparison
Scenario
Lean LaunchPilot launch
Base LaunchDedicated suite
Full LaunchMulti-course academy
Launch model
Use a partner clinic or rented classroom with the lightest fixed footprint.
Use a dedicated training suite with the model's full core setup.
Expand into a multi-course academy with more rooms and more teaching capacity.
Typical setup
Run small classes with shared space, minimal equipment, and a tight schedule.
Keep the clinical facility, core staff, and standard course mix.
Add instructors, more course dates, and larger support functions.
Cost drivers
Shared room rental
lower buildout
fewer staff
lighter working capital
Clinical facility rent
instructor payroll
compliance and insurance
core equipment
Extra training rooms
more instructors
higher marketing
larger equipment
working capital
Planning rangeCAPEX only
Low six figuresLowest footprint
Mid six figuresModel baseline
Upper six figuresScale build
Best fit
Best for a pilot launch or a local demand test.
Best for a local academy that wants control and repeatable scheduling.
Best for a regional platform with steady demand and deeper cash reserves.
!
Planning note: These scenario ranges are planning assumptions from the model, not exact quotes or vendor bids.
What are the biggest startup costs for a dermal filler training business?
Dermal Filler Injection Training is expensive because the real cost is safe, supervised training at scale, not the room. The biggest startup lines are qualified medical leadership, instructor pay, compliant clinical space, live hands-on supplies, insurance, and getting licensed clinicians into seats. In Year 1, payroll is about $580k, with $220k for the medical director, $165k for the lead instructor, and supplies taking 10% of revenue for injectable product plus 35% for medical consumables.
Core payroll costs
$220k medical director
$165k lead instructor
$75k operations coordinator
$65k admissions specialist
Space and supply costs
$12k monthly rent
$25k professional liability insurance
10% of revenue for product supply
35% of revenue for consumables
How should you fund a dermal filler training business financial plan?
Fund Dermal Filler Injection Training with enough cash to cover $1.605M in startup buildout spend and at least $791k through the Month 2 cash low point, and do it before signing leases or hiring full-time clinical staff. The base case shows $1.221M Year 1 revenue, $25k EBITDA, break-even in 2 months, and payback in 20 months. Here’s the quick math: the raise should track launch timing, seat capacity, pricing, instructor use, and runway, not just buildout.
Funding need
Cover $1.605M CAPEX
Hold $791k cash in Month 2
Fund before leases
Delay full-time staff
Model drivers
Use 65% occupancy
Assume 12 billable days monthly
Test $3,200, $4,500, $8,500 prices
Keep variable costs at 22%
How much money do you need to start a dermal filler training business?
You need $1,605k in upfront CAPEX for a Dermal Filler Injection Training business, plus a separate $791k minimum cash need in Month 2; see How Increase Dermal Filler Injection Training Profits? for the profit levers behind that gap. This plan assumes 12 billable days/month, 65% occupancy, courses at $3,200, $4,500, and $8,500, with breakeven in Month 2 and payback in 20 months; these are planning assumptions, not guaranteed quotes.
Cash Needed
Separate CAPEX: $1,605k
Month 2 cash need: $791k
Breakeven target: Month 2
Payback target: 20 months
Funding Drivers
Set class size and course mix
Choose location model and hands-on format
Model medical director structure
Review state-specific compliance costs
Key Takeaways
Separate lease runway from buildout cash needs.
Durable equipment creates a heavy upfront CAPEX load.
Payroll, oversight, and CME strain operating cash fast.
Consumables, insurance, and marketing scale with revenue.
Dermal Filler Injection Training Core Five Startup Costs
Clinical Training Space And Classroom Setup Startup Expense
Facility layout
A dermal filler training space needs a clean learner flow: reception, classroom seating, treatment rooms, storage, and sanitation zones. With $12k monthly rent and $18k monthly utility and medical waste services, the facility burns $30k a month before payroll and supplies. Keep any lease deposit in runway, not buildout.
Buildout CAPEX
Treat durable setup as CAPEX. The core hard costs here are $15k for office and reception furniture, $12k for surgical-grade lighting units, and $45k for clinical treatment stations, or $72k total. Price by quotes, room count, and whether live-model rooms must run at the same time.
Count learners per class.
Price simultaneous treatment rooms.
Separate rent from assets.
Cost control
The fastest way to trim this spend is to avoid overbuilding. If a partner clinic can host live models, you can cut room count and delay some CAPEX. If classes are small, one well-run treatment room may be enough. Don’t buy extra stations or lighting until you know learner flow and model schedule.
Use partner space first.
Stage lighting and seating later.
Match rooms to demand.
Sizing questions
Ask three things up front: how many learners per class, whether a partner clinic is available, and whether live-model rooms must run at once. Those answers decide rent, room count, and utility load. If the model schedule is staggered, the same space can do more work without adding another treatment bay.
Injectable Product, Consumables, And Model Support Startup Expense
Supply Base
This line item is bigger than it looks. The source model puts injectable product at 10% of Year 1 revenue and consumables at 35%, with a stated combined assumption of 135%; on $1.221M of revenue, that is about $1.648M a year before marketing and certification fees.
Opening Stock
Separate opening inventory from per-class cost. Count filler product, needles or cannulas, syringes, gloves, antiseptic, topical products, sharps disposal, emergency supplies, sanitation stock, and live-model support. Price it with units × unit cost × class count, plus any model fee, so the first order and ongoing class spend stay visible.
Per-Seat Spend
Control this cost by tracking supply intensity per seat, not just per course. A $8,500 private training seat can carry more product than a $4,500 advanced workshop seat, so class mix matters. Here’s the quick math: if seat-level supply runs high, margin drops fast even when seats are filled.
Cost Control
Keep waste down by buying to the schedule, not the shelf. Use vendor quotes, minimum stock levels, and model counts to set reorder points, and review disposal and sanitation usage after each class. What this estimate hides is fill rate risk: if seats slip, supply cost per learner jumps.
Medical Oversight, Instructors, And Curriculum Startup Expense
Curriculum Setup
Curriculum development, manuals, protocols, competency checklists, and CME readiness are pre-opening costs. Put recurring teaching fees and full-time payroll in operating costs or working capital instead. The clean split is one-time setup for course content and compliance, then ongoing spend for delivery and supervision.
Year 1 Payroll
Year 1 staffing includes $220k for the medical director and $165k for the lead aesthetic instructor, with operations, admissions, and clinical support bringing total payroll to $580k. That belongs in Year 1 cash planning, not startup CAPEX. Here’s the quick math: headcount drives burn, so class volume and seat fill must cover fixed labor.
CME And Staffing Model
Year 1 CME certification fees are modeled at 25% of revenue, so they scale with enrollment. If the instructor model shifts from contractor to full-time, cash burn rises but scheduling control improves. If you stay contractor-based, burn is lighter, but class timing depends on instructor availability.
Readiness Cost
Course manuals, competency checklists, and medical oversight should be finished before the first class so the academy starts with a ready-to-teach package. If those items slip into launch month, you create avoidable rework and delay revenue. Keep setup spend separate from monthly teaching payroll so the opening budget stays clean.
Equipment And Durable Training Assets Startup Expense
Durable gear total
The durable equipment line is the non-disposable setup. The listed items total $187k: $45k treatment stations, $25k advanced AV, $85k medical-grade refrigeration, $12k lighting, and $20k IT security. That is about 11.6% of the $1.605M CAPEX plan, before other fixed assets.
What to count
Count only assets that stay in the room: treatment stations, clinician stools if included, mirrors, sharps infrastructure, secure storage, medical refrigeration, laptops, AV gear, and simulation tools. Estimate each line with units × vendor quote, plus room count and any install fees. Keep disposable syringes, filler inventory, and monthly software out of this bucket unless they are capitalized.
Keep it lean
Buy to the class size you can fill now, not the one you hope for later. Phase noncritical AV and simulation gear if cash is tight, but do not cheap out on refrigeration, storage, or IT security. The common mistake is mixing in consumables, which makes the asset budget look bigger and less useful for cash planning.
Budget rule
This equipment subtotal belongs inside pre-opening CAPEX, not operating cost. If a line item gets used up in training sessions, it is a supply; if it stays on site and supports repeated classes, it is a durable asset. That split keeps the startup budget clean and makes financing asks easier to defend.
Insurance, Legal, Technology, And Enrollment Marketing Startup Expense
Fixed Spend
This cost bucket is heavy: recurring fixed spend is $28,950/month from $25,000 professional liability insurance, $3,000 legal and regulatory compliance, and $950 LMS/software. Add 6% of Year 1 revenue for digital acquisition and 25% CME certification fees, plus separate $35,000 LMS development CAPEX. State rules vary, so review each state separately.
Launch Stack
Build the budget from three inputs: months of coverage, Year 1 revenue, and vendor quotes. Count website, booking tools, CRM, photography, ads, waivers, refund policies, and consent forms in the launch stack. Keep the $35,000 LMS platform as CAPEX, not operating spend, so runway math stays clean.
Control It
Use one website, one booking flow, and one CRM at launch, then add features only after seats fill. Template the legal docs, but have counsel localize them by state before ads go live. The usual mistake is overspending on custom software before enrollment proves out.
State Checks
Do not treat licensure or compliance as uniform. Budget the $3,000/month legal line for state-specific review, plus consent language, waivers, and refund terms that match where you sell. That keeps enrollment campaigns moving without surprise rework when you expand beyond the first state.