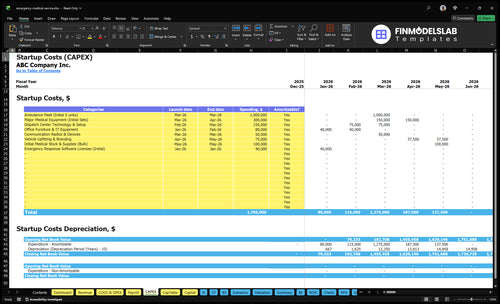
Emergency Medical Service Startup Costs: $145M Before Opening
This startup cost plan covers the startup period and first operating year for a US emergency medical service launch The researched model identifies $145 million of pre-opening CAPEX for 5 ambulances, major medical equipment, and dispatch setup, before working capital reserves These planning assumptions exclude ongoing operating losses unless noted and depend on state licensing, ALS versus BLS service level, station setup, insurance, staffing, and reimbursement timing
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets only for an emergency medical service, including fleet, equipment, and dispatch setup.
!
Exclusions Excludes payroll runway, fuel, insurance premiums, licensing renewals, deposits, inventory, working capital, debt service, and operating losses.
Calculate Fuding Needs
Startup Cost Summary
This table shows the main launch assets and the non-CAPEX cash reserve needed to start an emergency medical service.
Highlighted CAPEX$1,625,000Base planning example
Excluded cash needs$1,179,000Outside CAPEX total
Funding need$2,804,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Ambulance Fleet (Initial 5 units)
$1,000,000
Fleet count and vehicle spec
Yes
Major Medical Equipment (Initial Sets)
$300,000
Clinical equipment mix and readiness
Yes
Dispatch Center Technology & Setup
$150,000
Dispatch systems, install, and integration
Yes
Initial Medical Stock & Supplies (Bulk)
$100,000
Opening stock depth and supply mix
Yes
Vehicle Upfitting & Branding
$75,000
Ambulance buildout and launch prep
Yes
Operating Reserve
$1,179,000
Payroll runway and reimbursement timing
No
What does the Emergency Medical Service CAPEX screenshot show?
Costs rise fast as fleet size, clinical staffing, dispatch, and insurance move together. Lean trims the launch; Full adds depth, but some costs do not scale down cleanly.
Lean, Base, and Full launch cost bands for emergency response coverage.
Scenario
Lean LaunchSmaller fleet
Base LaunchModel baseline
Full LaunchBroader build
Launch model
Starts with a smaller fleet and a BLS-heavy response mix.
Uses the source model with five ambulances and the full core service mix.
Builds broader ALS, critical care, station, and dispatch depth.
Typical setup
Uses fewer ambulances, simpler dispatch, and lighter back-office staffing.
Keeps the priced fleet, equipment, dispatch, and admin team in place.
Adds more clinical coverage, more staffing depth, and stronger operating support.
Cost drivers
Ambulance units
basic equipment
dispatch and licensing
insurance
medical oversight
Five ambulances
equipment and radios
dispatch setup
fixed overhead
admin payroll
ALS and critical care staffing
station and dispatch support
insurance
training
fleet-ready equipment
Planning rangeCAPEX only
$600,000 - $900,000Lower capital
$1,700,000 - $2,000,000Core launch
$2,000,000 - $3,000,000Higher capital
Best fit
Fits founders testing demand with a smaller launch footprint and tighter cash control.
Fits operators launching the full modeled service without major trim to coverage or support.
Fits operators planning wider coverage and more complex emergency response from day one.
!
Planning note: Scenario ranges are researched planning assumptions from the model, not exact vendor quotes or bids.
What hidden costs come with starting an ambulance service?
Starting an Emergency Medical Service costs more than the ambulance itself because you also need insurance deposits, compliance setup, and cash to cover slow payer reimbursement; if you’re also sizing owner economics, see How Much Does The Owner Of An Emergency Medical Service Business Typically Make?. The hidden monthly burn can include $2,500 for general and professional liability insurance, $3,000 for fleet insurance, $15,000 for facility rent, $3,500 for dispatch and communication software, $1,200 for legal and accounting, and $33,750 for launch admin payroll, medical director oversight, credentialing, training, uniforms, compliance docs, and inspection fixes.
Upfront cash traps
Insurance deposits hit before revenue.
Compliance fixes come before launch.
Training and credentialing burn cash fast.
Uniforms and documents add setup spend.
Ongoing cash drain
60% of revenue can go to supplies.
40% can go to fuel and maintenance.
30% can go to billing fees.
Payer reimbursement delays strain working capital.
How do you fund an emergency medical service startup?
You fund an Emergency Medical Service startup by tying capital to the launch plan: licensing, fleet build, staffing, and a working capital runway long enough to survive slow collections. Lenders and investors usually want a startup budget, fleet plan, payer mix assumptions, a medical director agreement, licensing path, launch timeline, runway, and break-even forecast; model first-year prices of $1,800 for ALS, $950 for BLS, $700 for interfacility RN care, $1,500 for event medics, and $3,000 for critical care paramedics. Because modeled capacity runs 500% to 700% by service line, test slower collections and lower utilization.
What funders need
Startup budget with full launch costs
Fleet plan by unit and timing
Payer mix by revenue source
Medical director agreement signed early
Cash model checks
Licensing path with clear milestones
Launch timeline tied to spend
Runway for slow collections
Break-even forecast with low utilization
How much do ambulances cost for an EMS startup?
For Emergency Medical Service, plan on about $1,000,000 to start a 5-unit fleet, or roughly $200,000 per ambulance. Add another $300,000 for major medical equipment, or about $60,000 per unit if you spread it evenly, and keep maintenance reserves separate from acquisition capex.
Fleet buy-in
$1,000,000 for 5 ambulances
$200,000 per unit planning average
$300,000 extra for equipment
Keep reserves out of capex
Cost drivers
New versus used vehicles
ALS versus BLS setup
Remounts, stretchers, monitors
Oxygen, mileage, inspection readiness
Key Takeaways
Fleet acquisition can hit $1,000,000 for five units.
Medical gear needs $300,000 before restocking starts.
Licensing and oversight require permits, protocols, and $5,000 monthly.
Dispatch setup adds $150,000, plus monthly software and rent.
Emergency Medical Service Core Five Startup Costs
Ambulance Fleet Acquisition and Upfit Startup Expense
Fleet Buy Plan
The model treats ambulance fleet acquisition as the biggest CAPEX driver. It budgets $1,000,000 for 5 initial units in Month 3, or about $200,000 per ambulance before local specs. That figure shifts with ALS vs. BLS setup, reserve units, used mileage, remount needs, stretcher mounts, radios, markings, safety gear, and inspection readiness.
What To Include
Price each unit as more than a chassis. The upfit budget should cover stretcher mounts, radios, exterior markings, safety equipment, and anything needed to pass inspection at launch. Keep the vehicle buy separate from fuel, direct maintenance, and operating reserves; those are not CAPEX and are modeled at 40% of revenue in Year 1.
Count reserve units first.
Quote ALS and BLS separately.
Check remount and mileage.
Cut Risk
Trim cost by buying only the fleet mix you need on day one and using quotes tied to exact specs. Used units can save cash, but only if mileage, condition, and inspection readiness still hold. The mistake is underbuying safety gear or radio setup and paying later in delays, rework, or failed inspections.
Price by spec, not guess.
Protect inspection readiness.
Do not raid operating reserves.
Cash Timing
This spend lands early, so plan the cash draw before launch. If 5 units stay in the first wave, the model’s $1,000,000 fleet line should sit outside the Year 1 operating reserve, which covers fuel and maintenance. That split keeps vehicle purchases from distorting monthly burn.
Licensing, Inspections, and Medical Oversight Startup Expense
Licenses
Licensing is not one national fee. Budget for state EMS agency licensing, ambulance vehicle permits, inspections, protocols, a compliance manual, and any certificate-of-need review. The model also carries $60,000 in Year 1 for medical director oversight, or $5,000/month. Renewals belong in operating expense, not CAPEX.
Cost Inputs
This cost covers filing fees, inspection prep, controlled medication rules where allowed, and the medical director agreement. Build it from the number of states and local permits, fee quotes, and months of oversight needed. If you serve more than one jurisdiction, each permit and inspection line should be budgeted separately.
Control Risk
Keep the scope tight at launch. Start with the exact service area, collect the current state and local checklists, and get the medical director agreement signed before inspection dates. The main mistake is treating renewals or re-inspections as one-time setup costs. That hides real monthly burn.
Budget Rule
Put this line in startup cash, not equipment. Track one-time licensing fees, then carry the $5,000/month oversight cost in payroll or professional services. If controlled medications are in scope, add storage and rule review to the estimate. That keeps the budget aligned with actual compliance work.
Clinical Equipment and Onboard Supply Startup Expense
Equipment Budget
$300,000 is the planning pool for durable EMS gear across Months 3 to 4, or about $60,000 per initial ambulance if you spread it evenly. This covers stretchers, stair chairs, monitors, defibrillators, suction, oxygen, trauma supplies, PPE, and approved medication storage. Keep it separate from supplies and pharmaceuticals, which sit in Year 1 operating cost.
Per Unit Build
Price the loadout by ambulance, then test it with quotes. The key inputs are number of ambulances, unit prices, and months of coverage for starter stock. Use exact counts for stretchers, monitors, oxygen systems, and controlled storage, then add restocking inventory as a separate line.
Keep It Separate
Hold durable gear and consumables in separate buckets. Buy fixed equipment once, then budget medical supplies and pharmaceuticals at 60% of Year 1 revenue. That keeps startup cash clear and stops restocking from getting buried inside equipment capital spending (CAPEX). One clean rule: if it gets used up, it is not fleet CAPEX.
Budget Check
Pressure-test the budget by unit, not by hope. If the fleet starts with five ambulances, the equipment line works back to about $60,000 each, so any quote above that needs a clear reason. Lock the list early, because late adds like extra monitors or spare oxygen gear can push the total fast.
Facility, Dispatch, Communications, and Technology Startup Expense
Dispatch Setup
Dispatch center setup needs both one-time CAPEX and monthly run costs. The model sets aside $150,000 in Months 2 to 3 for technology and setup, then adds recurring launch overhead for rent, software, utilities, and admin support. This is where CAD, ePCR, billing, secure records, radios, and office IT get funded.
What It Covers
Budget this line for the facility and systems that let crews work and communicate. It should cover garage or station deposits, parking, crew quarters if needed, dispatch hardware, software, radios, CAD integration where applicable, ePCR, billing systems, secure records, and office IT. A clean estimate starts with quotes for setup plus monthly subscriptions.
$150,000 setup CAPEX
$15,000 rent per month
$3,500 software per month
Monthly Run Rate
Here’s the quick math: recurring launch overhead totals $21,000/month, made up of $15,000 rent, $3,500 software, $1,800 utilities and internet, and $700 admin supplies and services. That monthly run rate matters because it hits cash before collections do, so it belongs in startup funding, not just the income statement.
$1,800 utilities and internet
$700 admin supplies
$21,000 total monthly overhead
Keep Capex Separate
Don’t blur owned tech with subscriptions. Pay once for setup items like dispatch-center equipment and integration work, then track software, rent, utilities, and admin as monthly operating costs. That split keeps the budget honest, makes cash needs clear, and stops founders from underfunding the first few months of service launch.
Insurance, Hiring, Training, and Payroll Reserve Startup Expense
Payroll and Insurance Buffer
For launch, this is non-CAPEX cash, not equipment. The model carries $2,500/month general and professional liability insurance and $3,000/month vehicle fleet insurance, plus $405,000 in Year 1 admin and leadership payroll, or $33,750/month. That is $471,000 before hiring, training, and collections delay.
What to Fund
This reserve covers the early cash gap for recruitment, background checks, credentialing, uniforms, onboarding, training, workers’ compensation, and payroll before billing cash comes in. The salary plan includes an Operations Manager at $90,000, Billing and Collections Specialist at $60,000, HR and Administrative Coordinator at $55,000, Fleet and Logistics Manager at $75,000, Medical Director at 0.5 FTE of $120,000, and Lead Dispatcher at $65,000.
How to Control It
Keep insurance quotes current and size payroll to the launch schedule, not the long-term org chart. The clear math is $66,000 for 12 months of listed insurance, plus $405,000 in Year 1 payroll. What this estimate hides is launch timing, so delay hiring until each role supports live volume and compliance.
Runway Risk
If collections lag, this reserve gets consumed fast. A simple rule is to fund at least one full payroll cycle plus insurance before opening, then add extra runway for the hiring items that are not priced here. For an EMS launch, the labor plan is the cash pressure point, so timing matters as much as headcount.