Medical Practice Startup Costs: $670K First-Year Funding Plan
Medical Practice Bundle
Key Takeaways
Lease, build-out, and equipment drive startup spend.
Year 1 staffing totals $768,000 before payroll taxes.
Year 1 variable costs equal revenue.
Cash peaks near Month 5 at $670,000.
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates one-time capitalized startup assets only for a medical practice; the base case is $353,000 before contingency.
!
CAPEX only This calculator covers one-time capital purchases and leasehold improvements only. It excludes inventory, payroll runway, deposits, debt service, working capital, rent during ramp-up, marketing, credentialing delays, and other operating costs.
How do medical practice startup costs affect funding and projections?
For Medical Practice, startup costs drive both the loan size and the cash runway: the base model shows $353,000 of CAPEX and $670,000 of minimum cash, so the funding ask has to cover buildout plus operating cushion. With Month 2 breakeven, Year 1 EBITDA of $132,000, and $702,000 in Year 2, lenders will still want proof that provider ramp, visit volume, payer pricing, staffing, and reserves all hold up. Tie CAPEX to depreciation, startup spend to launch timing, and working capital to payer collections.
Funding math
$353,000 CAPEX base
$670,000 minimum cash
20-month payback
Loan plus owner equity
Model checks
Month 2 breakeven target
$132,000 Year 1 EBITDA
$702,000 Year 2 EBITDA
Collections and staffing timing
How much money do you need to open a medical practice?
You need at least $670,000 to open this Medical Practice, because the launch budget must cover more than equipment and build-out; see What Is The Main Goal You Aim To Achieve With Your Medical Practice? before sizing the funding ask. CAPEX is $353,000, fixed overhead is $21,700/month, and cash bottoms in Month 5 even though operating breakeven is modeled in Month 2.
Funding Need
$670,000 minimum cash by Month 5
$353,000 CAPEX for launch assets
$317,000 covers ramp-up and reserves
$21,700 monthly fixed overhead
Cash Timing
$768,000 Year 1 payroll before taxes
Plan around payer reimbursement lag
Track collections timing weekly
Use Month 5 as the checkpoint
What drives medical office build-out cost?
If you’re budgeting a $150,000 build-out for Month 1 through Month 5, the cost driver is the space scope, not just the contractor quote. For a Medical Practice, square footage, exam rooms, plumbing, electrical load, nurse station layout, waiting area, lab space, accessible restrooms, fire and life safety work, security, and landlord allowance do most of the damage. The first question is simple: is it second-generation medical space or raw office space?
Main cost drivers
Square footage sets the base.
Exam rooms raise fit-out needs.
Plumbing and electrical add hard costs.
Fire and life safety can’t be skipped.
Space and use check
Primary care needs less than specialty-ready space.
Procedure rooms add complexity fast.
Imaging can change the budget meaningfully.
Landlord allowance affects cash needed upfront.
Calculate Fuding Needs
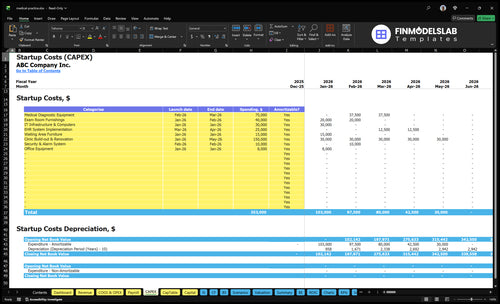
Startup cost summary
This table shows the main clinic startup assets and the non-CAPEX cash reserve needed at launch.
Highlighted CAPEX$320,000Base planning example
Excluded cash needs$670,000Outside CAPEX total
Funding need$990,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinic Build-out & Renovation
$150,000
Leasehold work, layout, and contractor scope
Yes
Medical Diagnostic Equipment
$75,000
Diagnostic device mix and installation needs
Yes
Exam Room Furnishings
$40,000
Room count, furniture grade, and setup
Yes
IT Infrastructure & Computers
$30,000
Devices, network gear, and setup work
Yes
EHR System Implementation
$25,000
Software setup, migration, and configuration
Yes
Working Capital Reserve
$670,000
Month 5 cash trough from payroll, rent, and overhead
No
Medical Practice Core Five Startup Costs
Facility Lease And Build-Out Startup Expense
Lease Setup
$12,000 monthly rent starts in Month 1, and the lease cash need also includes the security deposit and first month’s rent. Price the site from the lease term, tenant allowance, existing medical plumbing, and landlord delivery condition. Do not blend this with building purchase; that is a separate asset decision.
Build-Out Scope
The $150,000 build-out runs from Month 1 through Month 5 and should cover architectural work, contractor improvements, exam rooms, waiting area, nurse station, lab space, and compliance-ready finishes. If the shell already has medical plumbing, the quote should drop. Here’s the quick math: $30,000 per month over 5 months.
Ask for tenant allowance.
Reuse medical plumbing.
Confirm landlord delivery.
Cash Control
Carry costs add up fast: $1,500 utilities plus $1,200 cleaning each month, or $2,700 monthly before payroll, supplies, and other startup costs. Over the 5-month build-out window, that is $13,500. If occupancy starts early, keep cash tight and avoid overbuilding rooms you will not use in Year 1.
Monthly Carry
For the first 5 months, the facility cost base is $223,500 for rent, build-out, utilities, and cleaning, before deposits and professional fees. That gives you a clean target for funding talks and landlord negotiations, and it keeps the lease decision tied to actual occupancy needs.
Medical Equipment And Exam Room Startup Expense
Exam room base
Exam tables, sterilization gear, storage, and clinical fixtures are the core spend here. Plan the first wave as $40,000 for exam room furnishings in Month 1 through Month 2, plus $15,000 for waiting area furniture in Month 1 and $8,000 for office equipment in Month 1.
Diagnostics
Diagnostic equipment is the bigger ticket item at $75,000 in Month 2 through Month 3. Here’s the quick math: scope the number of devices, ask for quotes, and separate primary care essentials from specialty tools. That keeps the open budget tight and avoids paying for gear that sits idle early on.
Count rooms and devices needed
Quote each unit and install
Stage specialty gear later
Stage spend
The safest move is to buy only what supports year-one primary care, then delay specialty equipment until demand justifies it. A specialist physician is not added until Year 3, so buying a full specialty setup now ties up cash with no near-term use. Keep the first build lean and compliant.
Purchase order
Sequence orders by opening date: Month 1 for furniture and office gear, Month 2 through Month 3 for diagnostics, then hold specialty buys until patient volume and provider mix support them. That timing protects working capital while still giving the practice a clean, functional clinical setup.
EHR, Software, And IT Startup Expense
Hardware Base
$30,000 in Month 1 covers IT infrastructure and computers. Treat this as one-time setup, not a subscription. It should include the devices and network base needed for printers, scanners, phones, cybersecurity, and internet so the clinic can start on a clean system.
Software Spend
$25,000 for EHR implementation lands in Months 3 through 4, and recurring EHR and scheduling software is $2,000 per month. That cost should cover practice management, billing, patient portal, telehealth tools, and implementation training. Get quotes by module and seat count, not as one lump sum.
User Count
Year 1 should be sized to 7 users: 2 primary care physicians, 1 nurse practitioner, 2 medical assistants, 1 practice manager, and 1 front desk staff. Match licenses, logins, and training time to that team. One clean rule: buy only the seats you will use on day one.
Keep It Lean
Cut waste by staging extra modules until workflows are live. Start with charting, scheduling, billing, portal access, and telehealth, then add more only after go-live. The main mistake is paying for unused seats or features; the goal is to keep the $2,000 monthly run rate tied to real staff use.
Licensing, Credentialing, Insurance, And Professional Services Startup Expense
Licensing Cost
This bucket covers business formation, state registrations, medical board filings, Drug Enforcement Administration registration where needed, payer credentialing, legal review, accounting setup, and HIPAA compliance. There is no single licensing number, because cost shifts with state, specialty, provider count, and insurance structure. Use separate quotes for each item and treat delays as cash timing risk, not build cost.
Insurance Load
Budget $2,500 per month for malpractice insurance and $800 per month for general liability, then multiply by the months before launch and early operation. Add carrier fees and proof-of-coverage needs. This sits in startup overhead, not equipment, and it should be sized against provider count and services offered.
Multiply monthly premiums by launch months
Quote each carrier separately
Match coverage to services offered
Payer Timing
Payer credentialing drives cash more than most founders expect. In Year 1, billing and collections fees are 60% of revenue, so slow enrollment can choke cash flow fast. Use working capital for the gap between opening and first payments. Do not bury credentialing delays in CAPEX; they belong in cash planning.
Keep It Lean
Trim this cost by getting quotes early, bundling legal and accounting setup, and starting payer enrollment before launch. Ask carriers what licenses, board actions, and HIPAA documents they need, then stage renewals on a calendar. One clean line: paperwork is cheaper than a delayed first claim.
Staffing, Supplies, Marketing, And Working Capital Startup Expense
Working Capital
These costs belong in pre-opening expense and working capital, not CAPEX. Year 1 staffing is $768,000 before payroll taxes, with $1,000 per month for marketing and website, $700 per month for admin supplies, and medical supplies plus vaccines at 40% of revenue.
Staffing Load
Use the role list and salary rates to build the labor budget: 2 physicians at $220,000 each, 1 nurse practitioner at $110,000, 2 medical assistants at $45,000 each, 1 practice manager at $90,000, and 1 front desk staff at $38,000. That totals $768,000 in annual salary, before payroll taxes.
Supply Spend
Keep fixed admin spend light: $700 per month for office supplies and $1,000 per month for marketing and website. The big variable is clinical supply use, since medical supplies and vaccines run at 40% of revenue. So the clean estimate needs both a fixed monthly base and a revenue-linked cost rate.
Cash Cushion
Plan the launch around the cash trough, not just the opening date. Minimum cash reaches $670,000 in Month 5, so the startup budget needs enough runway to cover salaries, fixed overhead, and supply draws before collections catch up.
Compare 3 Startup Cost Scenarios
Startup cost scenarios
Startup costs move a lot with room count, provider mix, and equipment depth. Lean keeps the clinic small; Base matches the model; Full adds specialty readiness and more staffing.
Lean, Base, and Full launch bands for a medical clinic.
Scenario
Lean LaunchLower-capex start
Base LaunchModel base case
Full LaunchHigher-capex build
Launch model
A lean leased-office launch opens with a smaller footprint, fewer exam rooms, and a tighter provider mix.
A standard outpatient launch matches the model's core staffing and build-out.
A full launch adds specialty capacity, more providers, and procedure-ready space.
Typical setup
Use a simple clinic shell, basic furniture, core IT, and only the minimum equipment needed to start.
Use the modeled 2 primary care physicians, 1 nurse practitioner, 2 medical assistants, and the full core clinic package.
Use a broader provider team, added specialty equipment, procedure rooms, and deeper front-desk and clinical support.
Cost drivers
Smaller build-out
fewer exam rooms
lighter equipment package
lower staffing depth
Core build-out
2 primary care physicians and 1 nurse practitioner
2 medical assistants
full fixed overhead
Larger build-out
specialty equipment
procedure rooms
more providers
deeper staffing
Planning rangeCAPEX only
$800,000 - $950,000Lower funding band
$950,000 - $1,100,000Base funding band
$1,250,000 - $1,650,000Higher funding band
Best fit
Best for a solo or very small primary care start that wants to control cash burn.
Best for a standard primary care clinic that wants a balanced opening plan.
Best for a multi-provider clinic that wants specialty-ready capacity from day one.
!
Planning note: These scenario ranges are researched planning assumptions, not exact vendor quotes or bids.
This plan points to a $670,000 minimum cash need by Month 5, even with operating breakeven modeled in Month 2 That means the reserve must cover more than the $353,000 CAPEX budget It also needs room for $21,700 in monthly fixed overhead, payroll timing, payer collections, supplies, and billing fees during the early ramp-up period
The model reaches breakeven in Month 2 and payback in 20 months That is based on a Year 1 team of 2 primary care physicians, 1 nurse practitioner, 2 medical assistants, 1 practice manager, and 1 front desk employee Cash still bottoms in Month 5, so breakeven does not remove the need for working capital
Not in this base plan if the launch is primary-care focused The model starts with no specialist physician in Year 1 or Year 2, then adds 1 specialist physician in Year 3 The initial equipment budget includes $75,000 for diagnostic equipment and $40,000 for exam room furnishings, while specialty procedure equipment should be added only when the service line is staffed
Cut scope before cutting clinical readiness The largest source CAPEX line is the $150,000 clinic build-out, followed by $75,000 in diagnostic equipment and $40,000 in exam room furnishings A founder can stage specialty services, negotiate tenant improvements, reuse compliant medical space, and delay nonessential furniture while protecting patient care, billing, security, and compliance
Yes, lenders usually want the startup budget tied to revenue, staffing, cash runway, and repayment capacity In this plan, the key proof points are $353,000 in CAPEX, $670,000 minimum cash by Month 5, $132,000 Year 1 EBITDA, and 20-month payback They will also review provider ramp, visit volume, reimbursement assumptions, and monthly overhead
About the author
Adam Fletcher
Small Business Writer
Adam Fletcher is a small business writer at Financial Models Lab who researches how small businesses launch, operate, and earn money. He focuses on business affordability analysis and helps readers evaluate business ideas with a practical eye, especially when planning a business with limited capital. His work connects new ventures to realistic startup budgets in a clear, plain-spoken way for people starting out with less money.
Choosing a selection results in a full page refresh.