Functional Medicine Practice Startup Costs: $745K Funding Plan
Functional Medicine Practice
Key Takeaways
Build-out and reception start near $132K.
Equipment and furnishings add about $78K.
Tech setup needs $25K upfront plus $1.2K monthly.
Admin staffing alone runs $220K a year.
Functional Medicine CAPEX Calculator Objective
Startup CAPEX Calculator
Estimates the upfront capitalized startup assets for launch, not operating cash needs.
!
Exclusions This calculator covers only one-time capitalized startup assets. It excludes inventory, payroll runway, rent deposits, debt service, working capital, marketing, insurance premiums, financing costs, and other operating expenses.
How much money do I need to open a functional medicine practice?
You need about $745K to open a Functional Medicine Practice in this model, not just the $235K CAPEX for buildout and equipment. For owner earnings context, see How Much Does A Functional Medicine Practice Owner Make?; Year 1 shows $623K revenue and $238K EBITDA, while Month 1 breakeven and 15-month payback are model outputs, not guarantees.
Funding Need
$745K minimum cash need in Month 2
$235K CAPEX for setup and assets
Include deposits, setup, and pre-opening payroll
Fund the ramp-up period, not just launch
Launch Scale
Solo practitioner needs less staff funding
Small clinic matches the base model
Base team: physician, nurse practitioner, coach, dietitian
Multi-provider launch raises payroll and working capital
What is the biggest cost to start a functional medicine practice?
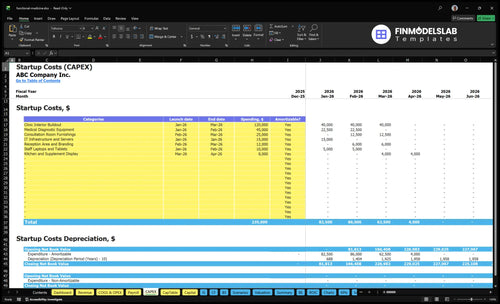
The biggest startup cost for a Functional Medicine Practice is usually clinical space build-out, but not always. In this model, the largest named CAPEX line is $120K for clinic interior buildout, while monthly fixed costs include $12K rent and $17,550 total fixed overhead, with $220K in Year 1 admin payroll before provider economics.
Cost drivers
Room count changes build cost fast
Lab draw needs add plumbing
Accessibility can raise finish costs
Patient experience drives signage and layout
Other big costs
Staffing readiness can outrun rent
EHR, telehealth, intake, billing, security matter
Technology costs rise with setup complexity
Cash runway covers slow patient ramp
How do you fund a functional medicine practice?
To fund a Functional Medicine Practice, lenders need a plan that ties startup uses of funds, CAPEX, and cash runway to real visit volume and staffing. This model shows $623K Year 1 revenue, $1.309M Year 2 revenue, $235K CAPEX, and a $745K minimum cash need, with 15-month payback. The math works only if your provider schedule and pricing hit plan.
Revenue bridge
Physician: 80 monthly treatments at $450
Nurse practitioner: 100 monthly at $325
Health coach: 120 monthly at $150
Registered dietitian: 110 monthly at $200
Funding plan
$235K CAPEX must be scheduled
$745K minimum cash need sets runway
1217% IRR and 879% ROE drive the pitch
Validate assumptions before borrowing
Startup Cost Summary Table Objective
Startup cost summary
Summarizes startup assets and the non-CAPEX cash needed to cover the Month 2 trough.
Highlighted CAPEX$217,000Base planning example
Excluded cash needs$745,000Outside CAPEX total
Funding need$962,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinic Interior Buildout
$120,000
Leasehold improvements, fit-out scope, and finish level
Yes
Medical Diagnostic Equipment
$45,000
Diagnostic room equipment package and supplier mix
Yes
Consultation Room Furnishings
$25,000
Number of rooms and furniture quality
Yes
IT Infrastructure and Servers
$15,000
Servers, devices, and telehealth setup
Yes
Reception Area and Branding
$12,000
Front desk finish, signage, and brand package
Yes
Opening cash buffer
$745,000
Month 2 cash trough, $17,550 fixed monthly costs, and $220,000 Year 1 admin payroll
No
Functional Medicine Practice Core Five Startup Costs
Clinical Space and Build-Out Startup Expense
Build-Out Scope
This covers the clinic shell and patient-facing finish-out: lease deposit, consult rooms, exam rooms, accessibility, patient flow, signage, plumbing, electrical work, and any lab draw area. The source model uses $120K for interior build-out from Month 1 to Month 3, plus $12K for reception and branding, and $12K monthly rent.
Cost Drivers
Estimate this with three inputs: landlord allowance, square footage, and room count. Building condition and patient experience standards move the number fast. A newer shell usually needs less work; older space can push costs up. Treat this as a planning estimate, not a contractor quote, and confirm whether lease deposits are included.
Landlord allowance changes cash need.
Room count drives walls and utility work.
Lab draw setup adds cost.
Save Without Cutting Quality
Use the landlord allowance first, then phase nonessential finishes after opening. Keep the room layout simple, and only add a lab draw area if the launch needs it. The big mistake is overbuilding for a perfect patient experience before demand is proven. The goal is a clean, compliant space that works on day one.
Ask for tenant improvement dollars.
Standardize room layouts.
Delay cosmetic upgrades.
Budget Fit
This line is mostly upfront cash, while rent is recurring overhead. It sits next to equipment, tech, licensing, and staffing in the launch budget. If the landlord funds part of the finish-out, cash pressure drops, but the space still has to support accessibility, clear patient flow, and the clinical setup you plan to open with.
Medical Equipment and Clinical Setup Startup Expense
Core Gear
A functional medicine setup can start with the basics plus selective specialty tools. The model uses $45K for medical diagnostic equipment, $25K for consultation room furnishings, and $8K for kitchen and supplement display, or about $78K total. This can cover exam tables, vitals equipment, scales, refrigeration, workstations, and waiting room furniture.
What Counts
Estimate it by room count, equipment list, and unit quotes. Ask first: does the launch include lab draws, supplement sales, advanced diagnostics, or consult-only care? Then price exam tables, blood pressure cuffs, scales, phlebotomy supplies if needed, and fridges. This line item is one of the biggest early cash uses, so it should match the care model.
Count rooms before buying.
Price each item by quote.
Separate basics from specialty gear.
Trim It
Keep the first build focused on required clinical basics: exam furniture, vitals tools, scales, and secure storage. Add specialty devices only when the service menu needs them. The usual mistake is buying advanced diagnostics before patient volume proves the use case. If you do not plan lab draws or supplement retail, skip those pieces at launch.
Buy for current services.
Delay nonessential devices.
Match gear to rooms.
Launch Mix
For a lean opening, the spend should reflect the visit type. Consult-only care needs less hardware than a lab-enabled clinic, and supplement retail adds shelving, refrigeration, and display space. The right budget starts with the service list, then maps each room, device, and workstation to a quote. That keeps the plan tight and avoids dead inventory.
Healthcare Technology and Digital Infrastructure Startup Expense
Tech budget
$15K for IT infrastructure and servers plus $10K for staff laptops and tablets puts the upfront digital setup at $25K. Add $1,200/month for EHR and telehealth software, so year-one tech spend is about $39,400 before any extra vendor fees.
What it covers
This budget covers the core clinic stack: electronic health record, scheduling, billing, telehealth, patient portal, secure messaging, online intake forms, website, payment processing, phones, cybersecurity basics, and backup access. Plan it as one-time setup plus recurring subscriptions, not one blended number.
Separate setup from monthly fees
Budget for HIPAA-compliant communications
Confirm backup access before launch
Keep it lean
Ask vendors for a single quote that shows setup, monthly software, and any add-ons. HIPAA-compliant communications can push cost up fast, so only pay for features your team will use on day one. Common waste: buying more seats, modules, or devices than staff need.
Buy only active user licenses
Test workflow before adding tools
Skip nonessential add-ons at launch
Launch timing
Implementation time affects launch readiness. If software setup, migration, and staff training run long, the clinic may have hardware in place but still not be able to see patients, take payments, or message securely, so start vendor onboarding early and test every workflow before opening.
Licensing, Compliance, Insurance, and Professional Services Startup Expense
Licensing setup
Licensing, compliance, and insurance can swing hard by state and provider type, so treat this as a planning line, not a quote. The source model uses $2,500 per month for professional liability insurance, while setup work can include entity formation, legal review, credentialing, HIPAA policies, OSHA basics, and payer enrollment if needed.
What it covers
This bucket covers the paperwork and controls needed to open safely: state medical requirements, compliance documentation, general liability, accounting support, and payer setup if you bill insurance. The key inputs are state rules, provider mix, clinical services, and whether you take payers. Setup fees are one-time; insurance and compliance support keep running.
Entity formation and legal review
HIPAA and OSHA basics
Payer enrollment, if applicable
How to budget it
Here’s the quick math: $2,500 monthly professional liability insurance equals $30,000 a year before deductibles or extra coverages. Keep one-time legal and credentialing costs separate from monthly premiums and ongoing compliance retainers, so you don’t understate launch cash needs. If your model is cash-pay only, payer enrollment costs may be lower.
Separate setup from recurring costs
Ask for state-specific quotes
Update after service scope changes
Budget risk
What this estimate hides is scope creep: adding lab draws, expanding payer billing, or changing clinical services can raise compliance work fast. For a tighter launch, get separate quotes for insurance premiums, legal retainers, and credentialing, then refresh the budget whenever your state filing or provider mix changes.
Staffing, Training, Inventory, and Launch Readiness Startup Expense
Pre-Open Payroll
To open the clinic, budget $220K a year for admin staff: 1 practice manager at $85K, 1 patient coordinator at $50K, 1 medical assistant at $45K, and 1 receptionist at $40K. That covers hiring, onboarding, and front desk readiness before visits start.
Launch Team Setup
Clinical launch staffing includes 1 physician, 1 nurse practitioner, 1 certified health coach, and 1 registered dietitian. Add time for credentialing, front desk setup, medical assistant readiness, initial supplements, office supplies, and launch marketing. Those are pre-opening cash needs, not steady-state payroll.
Budget credentialing time
Stock first-month supplies
Separate launch marketing
Protect Cash Burn
Keep pre-opening expense separate from ongoing operating cost. One-time startup cash should cover onboarding, setup, and opening inventory, while the $220K admin payroll becomes part of the run rate after launch. That split makes month-one cash burn easier to track and fund.
Pre-Opening Cash Plan
Use a launch budget for hiring, training, credentialing, and opening supplies, then move only the live payroll into monthly operating costs. If those pre-launch tasks slip, cash tied up in people and inventory rises before the first patient visit.
Lean, Base, and Full Functional Medicine Startup Budget Scenarios
Scenario table
Larger rooms, heavier staffing, and more working cash push startup cost from a lean telehealth-first setup to a full clinic build.
Lean, base, and full launch cost comparison for a Functional Medicine Practice.
Scenario
Lean LaunchLean setup
Base LaunchCore clinic
Full LaunchExpanded build
Launch model
Start with consult-led visits and telehealth support, keeping the physical footprint small.
Open one physician-led clinic with a care team and steady in-person visits.
Open a larger clinic with multiple rooms and multiple providers from day one.
Typical setup
Use one provider, basic software, and minimal exam room space.
Use one physician plus support staff, standard equipment, and one central location.
Use deeper equipment, more staff, and more working cash for ramp-up.
Cost drivers
Telehealth setup
light buildout
core software
limited equipment
opening cash
Clinic buildout
diagnostic equipment
core staff
monthly overhead
working capital
More rooms
deeper equipment
higher payroll
more inventory
bigger working cash
Planning rangeCAPEX only
$150,000 - $350,000Lower buildout
$235,000 - $745,000Core clinic
$745,000 - $1,100,000Higher cash need
Best fit
Fits founders testing demand before committing to a larger clinic.
Fits operators building a stable local practice with measured growth.
Fits teams with capital and a plan to scale patient volume fast.
!
Planning note: These ranges are researched planning assumptions, not exact quotes; actual US market costs vary by city, room count, staffing mix, and vendor pricing.
The model’s minimum cash need is $745K in Month 2, so the reserve must cover more than equipment It needs to absorb $235K of CAPEX, $176K of monthly fixed overhead, and Year 1 admin payroll of $220K If credentialing, hiring, or patient acquisition runs slow, working capital gets tight fast
This model reaches breakeven in Month 1 and pays back in 15 months, but that result depends on hitting volume and price assumptions Year 1 revenue is $623K, supported by 80 physician treatments at $450 and 100 nurse practitioner treatments at $325 per month A slower ramp pushes payback later
Not always, but this model includes supplement inventory as a revenue-linked cost starting in Month 1 The assumption is 50% of revenue in Year 1, falling to 40% by Year 3 If you skip supplement sales, you may reduce inventory needs, but you may also change visit economics and patient care workflows
The best model depends on services, state rules, patient expectations, and provider workflow This plan assumes leased space with $12K monthly rent, $120K interior buildout, and $45K diagnostic equipment A telehealth-heavy launch may cut build-out and equipment, but it still needs compliant software, insurance, intake, billing, and patient acquisition
Staffing is a major cash driver because payroll starts before full patient volume The Year 1 admin team costs $220K annually across a practice manager, patient coordinator, medical assistant, and receptionist The clinical plan also starts with 1 physician, 1 nurse practitioner, 1 health coach, and 1 registered dietitian, so onboarding and scheduling discipline matter
About the author
Jack Bennett
Business Model Writer
Jack Bennett is a business model writer at Financial Models Lab, where he explains startup planning and business model economics in clear, practical language. He focuses on the money questions new founders ask when comparing business ideas, with an eye on how small businesses operate day to day. Jack’s writing helps readers understand the numbers behind real business operations without heavy finance jargon, making complex decisions feel more manageable and grounded.
Choosing a selection results in a full page refresh.