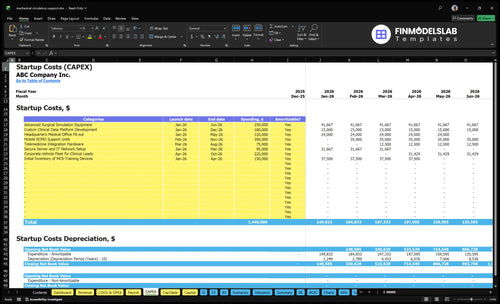
Mechanical Circulatory Support Startup Costs: $129M+ CAPEX
Use $129M in known CAPEX as the researched opening benchmark for this Mechanical Circulatory Support Services plan, before adding launch payroll, compliance work, inventory timing, and working capital In the first operating year, the model also carries $109M in salaries, $5064k in fixed overhead, and revenue-linked costs equal to 185% of revenue These are planning assumptions, not vendor quotes, and total funding still depends on facility design, device scope, payer timing, and reserve policy
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets only for a mechanical circulatory support service, so you can size the buildout before adding runway or other cash needs.
!
Excluded from CAPEX Not included: pre-opening payroll, training expense, licenses, consumed case inventory, deposits, working capital, debt service, financing costs, or operating expenses. Model those separately.
Calculate Fuding Needs
Startup cost summary
Shows startup CAPEX and excluded cash needs for a cardiac mechanical circulatory support service.
Highlighted CAPEX$1,050,000Base planning example
Excluded cash needs$704,000Outside CAPEX total
Funding need$1,754,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Advanced Surgical Simulation Equipment
$250,000
Training lab and simulation setup
Yes
Mobile ECMO Support Units
$350,000
Transportable support units and bedside coverage
Yes
Custom Clinical Data Platform Development
$180,000
Registry workflow and data capture buildout
Yes
Headquarters Medical Office Fit-out
$120,000
Clinical space buildout and room readiness
Yes
Initial Inventory of MCS Training Devices
$150,000
Training-device stock and launch inventory
Yes
Operating Cash Reserve
$704,000
Payroll burn, reimbursement lag, and inventory float
Costs rise fast as you move from a small hospital pilot to a full platform because more device types, deeper call coverage, inventory, and reserve use all add cash demand.
Lean, Base, and Full launch cost comparison
Scenario
Lean LaunchHospital pilot
Base LaunchIntegrated center
Full LaunchAdvanced platform
Launch model
Start with a limited temporary support service using existing facilities and a narrow device set.
Run a fully integrated cardiac program with the device mix and staffing in the model.
Expand into broader heart failure and circulatory support coverage with more device types and call burden.
Typical setup
Use one care path, lower backup capacity, and a smaller working capital reserve.
Use the modeled clinical team, fitted-out headquarters, core software, and steady operating reserves.
Add deeper on-call coverage, more training load, larger inventory, and a bigger reimbursement reserve.
Cost drivers
Existing facility use
fewer device categories
lower backup staffing
smaller inventory
modest reserve
Full capex buildout
clinical salaries
fixed overhead
revenue-linked costs
compliance systems
Broader device mix
deeper call coverage
heavier training
larger inventory
reimbursement reserve
Planning rangeCAPEX only
$900,000 - $1,400,000Lowest cash need
$1,400,000 - $2,200,000Modeled build
$2,000,000 - $3,200,000Highest cash need
Best fit
Best for a hospital pilot that wants to prove demand before scaling.
Best for an integrated cardiac center that wants the modeled Year 1 scale.
Best for an advanced heart failure platform with multi-site support needs.
!
Planning note: Ranges are researched planning assumptions based on the model, not exact quotes.
How much funding is needed for a mechanical circulatory support program?
Mechanical Circulatory Support Services needs more than equipment money: plan for $129M of CAPEX, plus $109M in Year 1 salaries and $5.064M in fixed overhead, before you count pre-opening expenses, inventory timing, reimbursement lag, case ramp, and a working capital reserve. Here’s the quick math: modeled Year 1 revenue is about $436M, and the first-month run-rate revenue is about $363k if the monthly assumptions hold.
Funding stack
$129M CAPEX is known
$109M Year 1 salaries
$5.064M fixed overhead
185% variable cost burden
Modeled revenue
Year 1 revenue: about $436M
Cardiac surgeon: about $193M
Heart failure cardiologist: about $979k
VAD coordinator: about $756k
Perfusionist: about $507k
Clinical data specialist: about $180k
How much does it cost to open a mechanical circulatory support service?
Opening Mechanical Circulatory Support Services is not a universal quote; the modeled planning budget starts at $129M in known CAPEX, plus $109M in Year 1 salary load and $5.064M in fixed overhead. For funding logic, see How To Write A Business Plan For Mechanical Circulatory Support Services?, because scope shifts fast when adding temporary MCS, durable VAD coordination, ECMO, or broader advanced heart failure coverage.
Core cost stack
$129M known CAPEX planning base
$109M Year 1 salary load
$5.064M fixed overhead
Facility integration can move funding materially
Capacity ramp
Cardiac surgeons ramp at 65%
Heart failure cardiologists ramp at 60%
VAD coordinators ramp at 70%
Perfusionists 60%; data specialists 50%
What are the biggest cost drivers for a mechanical circulatory support program?
For Mechanical Circulatory Support Services, the biggest cost drivers are capital equipment, backup capacity, and the clinical systems around them. The largest identified CAPEX line is $350k for mobile ECMO support units, followed by $250k for advanced surgical simulation equipment, and the listed items total about $1.29M. In this setting, redundancy is not optional: emergency cardiac support cannot depend on one unit, one trained person, or one pathway.
Largest CAPEX lines
$350k mobile ECMO support units
$250k surgical simulation equipment
$220k clinical lead vehicle fleet
$180k custom clinical data platform
Support costs that matter
$120k office fit-out
$95k secure server and IT network
$75k telemedicine hardware
Service contracts protect uptime and response speed
Key Takeaways
Separate equipment CAPEX from starter inventory and disposables.
Existing-hospital upgrades cost less than new clinical space.
Compliance needs setup plus ongoing legal, registry overhead.
Year 1 staffing and training drive the largest burn.
Mechanical Circulatory Support Services Core Five Startup Costs
Mechanical Circulatory Support Equipment Startup Expense
CAPEX anchor
Keep durable equipment separate from implants and disposables. Start with $350k for a mobile ECMO support unit and $250k for advanced surgical simulation equipment, then add consoles, controllers, monitors, backup units, emergency readiness gear, and biomedical installation. That puts the visible equipment floor at $600k before site-specific add-ons.
Sizing inputs
Build this line from how many support locations, backup units, and emergency transport needs the program must cover. Ask for vendor quotes on support systems, training devices, and biomedical installation, then price each unit separately. If quotes are pending, keep initial MCS training devices as a quote-dependent inventory item, not a fixed CAPEX number.
Keep it lean
Don’t buy duplicate backup gear before you know call volume and transport coverage. A shared emergency pool, phased purchases, and bundled installation can trim waste without cutting readiness. One-line rule: buy for the coverage you must prove, not the coverage you hope to grow into. Keep training devices separate until the vendor quote is final.
Starter inventory split
Keep launch stock outside CAPEX. Put unpriced MCS training devices in a separate starter inventory budget until quotes arrive, then split starter stock, reorder reserve, and emergency replacements into their own lines. That keeps the equipment ask clean and stops disposable case inventory from being mixed into startup hardware.
Mechanical Circulatory Support Accreditation and Compliance Startup Expense
Compliance setup
Startup compliance for mechanical circulatory support covers clinical protocols, privileging, quality reporting, payer enrollment, hospital accreditation prep, Centers for Medicare & Medicaid Services (CMS) requirements, legal review, documentation systems, and registry readiness. This is planning content, not legal or regulatory advice, so confirm scope with counsel, accrediting bodies, facility leadership, and payer enrollment teams.
Budget lines
The main setup line is $45k for registry and compliance software. Add one-time work for policy drafting, template documents, mock survey prep, and registry onboarding. Use vendor quotes, number of sites, and existing hospital workflows to size the build. That keeps setup costs separate from ongoing compliance overhead.
Protocol and privileging files
Payer enrollment packet prep
Registry build and testing
Run-rate overhead
Ongoing overhead is the part that keeps running after launch: $8k a month for legal and regulatory oversight, or $96k a year if steady for 12 months, plus the $115kYear 1 quality and registry manager salary. One line is setup, one line is run-rate, and mixing them hides the real burn.
Approval gate
Do not open the program until counsel, the accrediting body, facility leaders, and payer enrollment teams sign off on the protocol set, documentation flow, and registry plan. The software and staffing line only works if those approvals are in place before launch.
Mechanical Circulatory Support Facility Buildout Startup Expense
Site Readiness
Facility cost is site-specific. Build it around procedure room readiness, ICU integration, power and backup systems, sterile handling, infection control, storage, equipment parking, and patient flow. The known readiness line is $120k for headquarters medical office fit-out. Ask first: does this sit inside an existing cardiac program, or does it need major renovation?
Separate existing-hospital upgrades
Separate new clinical space
Price each room and system
Cost Inputs
Use two buckets: upgrade costs for an existing hospital site, and buildout costs for new or expanded space. Get quotes for square feet, room count, electrical and backup systems, clean storage, and ICU-adjacent workflow. The model should not use one universal estimate, because facility scope changes fast with infection control and patient movement needs.
Count procedure rooms
Count backup units
Measure square feet
Keep It Lean
Control spend by using existing cardiac space when possible, phasing work, and getting facility, ICU, and engineering sign-off before leasing or construction. The $120k office fit-out is only one line. What this estimate hides is the big swing from minor upgrades to full renovation, so price those separately.
Separate the Scope
For planning, keep existing-hospital upgrade costs apart from new or expanded clinical space. That split keeps the budget honest and stops a small office fit-out from masking the real cost of procedure rooms, ICU integration, sterile flow, and backup power.
Mechanical Circulatory Support Staffing and Training Startup Expense
Ramp-Up Team
Pre-opening staffing is the real burn here: recruitment, onboarding, proctoring, simulation, device training, call coverage planning, ICU nurse education, perfusion support, VAD coordinator readiness, and admin coordination. The Year 1 clinical service plan assumes 4 cardiac surgeons, 4 heart failure cardiologists, 8 VAD coordinators, 4 perfusionists, and 2 clinical data specialists.
Cost Inputs
Estimate this with headcount × ramp-up months × loaded pay, then add training travel, proctor time, and backfill coverage. The corporate Year 1 salaries named here total $1.43M: $450k Chief Medical Officer, $220k VP of Hospital Relations, $185k Director of Clinical Operations, $115k Quality and Registry Manager, $85k Billing and Coding Specialist, and $375k Human Resources Coordinator.
Count months before live cases
Price proctoring and simulation
Add call-coverage backfill
Trim Safely
Cut cost by staging hires, sharing coverage across sites, and using train-the-trainer sessions instead of one-off sessions. Keep ICU nurse education and device training intact, because weak onboarding raises errors fast. The clean savings lever is fewer paid ramp-up months, not thinner clinical readiness.
Coverage Readiness
What this estimate hides is the cost of keeping the program safe before volume arrives: call schedules, cross-coverage, and last-minute admin work. If the team starts too lean, overtime and locum-style backfill can erase savings. The model’s stated Year 1 salary load is $109M, so the budget needs a hard ramp plan, not hopeful staffing.
Mechanical Circulatory Support Initial Inventory and Maintenance Startup Expense
Launch stock
Separate launch inventory from ongoing burn. Opening stock should cover disposables, cannulation-related supplies, sterile packs, and emergency replacements for the first cases. Add quote-based MCS training devices as separate capital spending (CAPEX) or inventory. Size it with units × unit cost × coverage months, so the startup budget shows stock, not service cost.
Per-case burn
In the model, Medical Consumables and Sterile Kits are 45% of Year 1 revenue and ease to 35% by Year 5. That is per-case burn, not opening stock. Malpractice is another 65% of Year 1 revenue, but it is an operating allocation, not physical inventory. Keep those lines separate when you size startup cash.
Match stock to case volume.
Quote every consumable line.
Hold emergency reserve stock.
Cost control
To keep cost down, match kit counts to the procedure plan, standardize pack contents, and reorder only against actual use. Keep emergency stock small and visible. One clean one-liner: if it isn’t on the case cart or in the service contract, don’t park it in inventory.
Standardize sterile pack contents.
Track waste and expiry.
Separate maintenance from stock.
Readiness reserve
Add vendor service agreements, preventive maintenance, biomedical testing, and readiness checks as a separate reserve. Quote the initial MCS training devices if vendor pricing is pending, and keep emergency replacements outside launch stock. That keeps the startup budget clean: stock, per-case burn, and uptime support each sit in its own line.