Mobile Health Clinic Startup Costs: Plan $580K CAPEX Plus Cash Reserve
Mobile Health Clinic
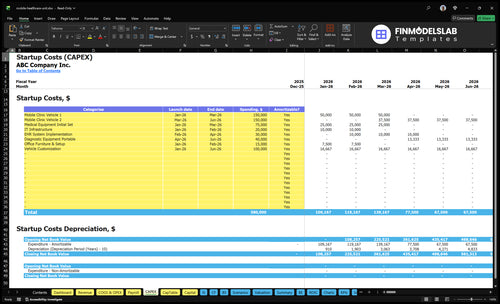
The researched mobile health clinic startup cost is $580,000 in capital assets before working capital, soft costs, and financing needs The largest startup items are $300,000 for two mobile clinic vehicles, $100,000 for vehicle customization, $115,000 for medical and diagnostic equipment, and $50,000 for IT and EHR setup Total funding need is higher than CAPEX alone because the model also carries a $486,000 minimum cash requirement in Month 6 These assumptions are planning estimates, not vendor quotes or guarantees
Estimate Startup Costs with Calculator
Startup CAPEX
Estimate capitalized startup assets only for a mobile health clinic, including vehicles, upfit, equipment, and setup costs.
!
CAPEX only This calculator covers capital assets only. It excludes inventory, payroll runway, deposits, debt service, working capital, marketing, insurance premiums, transaction fees, and other operating costs.
How much money do I need to start a mobile health clinic?
You likely need more than $400,000 to start a Mobile Health Clinic; the researched asset budget is $580,000 CAPEX, and the reserve marker is $486,000 minimum cash in Month 6, so planning around the vehicle purchase alone is too thin. For KPI tracking once you launch, tie spending to visits, payer mix, and collections using What Strategies Are You Using To Measure The Success Of Mobile Health Clinic?, because reimbursement timing can turn a funded clinic into a cash crunch.
Startup Cash Stack
$300,000 vehicle purchase line
$400,000 vehicle plus customization spend
$580,000 researched CAPEX asset budget
$486,000 Month 6 minimum cash reserve
Operating Burn
$18,750 fixed overhead per month
$265,000 annual admin wages
$40,833 monthly base before clinical costs
Cost shifts with scope, staffing, state rules
How should I fund a mobile health clinic startup budget?
Fund the Mobile Health Clinic in two buckets: $580,000 CAPEX for vehicles and equipment, then working cash for payroll, insurance, fuel, supplies, billing lag, and grant delays. Use equipment loans, vehicle financing, grants, donations, and owner equity for the build, and plan for about $40,833 a month in fixed payroll and overhead plus $8,000 in vehicle lease or loan payments. A practical financial model should tie CAPEX, startup expenses, launch timing, reimbursement timing, grants, debt assumptions, depreciation, and cash runway, with $486,000 minimum cash by Month 6.
Build funds
$580,000 CAPEX target
Use equipment loans first
Use vehicle financing too
Fill gaps with owner equity
Protect cash
Cover $40,833 monthly base costs
Add $8,000 vehicle payments
Hold $486,000 by Month 6
Model reimbursement and grant delays
What hidden costs come with starting a mobile health clinic?
The hidden cost in a Mobile Health Clinic is not just the vehicle—it’s the cash needed before the first visit and while claims are still unpaid. If you're sizing How Much Does The Owner Of Mobile Health Clinic Make?, the listed recurring fixed base is $7,450/month from $3,000 vehicle insurance, $1,200 professional liability, $750 legal and compliance, $1,000 EHR, and $1,500 marketing, plus a 15% Year 1 variable load for supplies, fuel, maintenance, and billing fees. The real squeeze is working capital, because launch payroll, fuel reserve, maintenance reserve, and supply inventory all hit before collections do.
Before opening
State licensure and clinical protocols
Legal setup and accounting setup
Billing setup and privacy policies
Staff onboarding and credentialing
After launch
$3,000 vehicle insurance monthly
$1,200 professional liability monthly
$1,000 EHR plus billing fees
15% variable load on revenue
Calculate Fuding Needs
Startup cost summary
This table groups launch CAPEX and separate non-CAPEX cash need into low, base, and high scenarios.
Highlighted CAPEX$580,000Base planning example
Excluded cash needs$486,000Outside CAPEX total
Funding need$1,066,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Mobile clinic vehicle acquisition
$300,000
Two clinic vehicles
Yes
Vehicle conversion and upfit
$100,000
Medical buildout and customization
Yes
Initial medical equipment
$75,000
Exam and treatment equipment
Yes
Portable diagnostic equipment
$40,000
Testing and point-of-care devices
Yes
IT, EHR, and office setup
$65,000
Systems, software, and setup
Yes
Operating cash reserve
$486,000
Month 6 cash floor and launch timing gap
No
Mobile Health Clinic Core Five Startup Costs
Vehicle Acquisition and Conversion Startup Expense
Vehicle CAPEX
The biggest startup swing is the vehicle and upfit. A base budget of $400,000 assumes 2 mobile clinic units at $150,000 each plus $100,000 for customization. That covers purchase or lease down payment, structural conversion, exam layout, cabinetry, power, HVAC, plumbing, generator, refrigeration, accessibility, storage, privacy, and maintenance readiness.
What It Includes
Here’s the quick math: 2 × $150,000 + $100,000 = $400,000. Use that line item only after you confirm vehicle count, service mix, route type, and daily stop volume. If the unit must support vaccine refrigeration, lab draws, or point-of-care testing, the build changes fast and so does the budget.
Confirm vehicle count first
Match build to service scope
Check power and cooling load
Control The Spend
Keep the unit as simple as the care model allows. Rural routes, ADA access needs, and storage for privacy or refrigeration can justify heavier specs, but avoid paying for features you won’t use. The common mistake is buying for every possible service instead of the actual daily stop count and exam workflow.
Price the build from use cases
Skip unused equipment bays
Review maintenance readiness early
Sizing Questions
Start with the route, not the truck. Ask how many vehicles you need, whether the mix is primary care or screening-heavy, how far the unit travels, how many stops it makes per day, and whether it must handle generator load, vaccine storage, lab draws, or point-of-care testing. Those answers set the real capex floor.
Medical Equipment and Supplies Startup Expense
Core gear
For a mobile clinic, the core equipment budget is $115,000: $75,000 for fixed medical equipment and $40,000 for portable diagnostics. That should cover exam tables, vaccine refrigeration, point-of-care testing, PPE, sharps disposal, emergency gear, phlebotomy, chronic care tools, and women’s health add-ons.
Budget math
Here’s the quick math: estimate units × unit price, then add quotes for delivery, setup, and calibration. Year 1 supply use should track revenue, not wishful stocking: 6% of revenue for medical supplies and pharmaceuticals, plus 3% for diagnostic test kits. Service scope and licensing decide what devices you actually need.
Right-size it
Don’t buy a generic clinic wish list. If you won’t do lab draws, women’s health, or on-site point-of-care tests, the gear list and storage plan should shrink fast. Referral workflows matter too, because some patients only need stabilization, screening, and handoff to a partner site.
Spend control
The cleanest savings come from matching equipment to route mix and licensing. Rural routes may need more self-contained gear; urban stops may need faster turnover. Cut waste by standardizing one base kit per vehicle and adding only the specialty items your service line and permit set require.
Compliance, Licensing, Insurance, and Professional Setup Startup Expense
State setup
State rules drive the first compliance bill. A mobile clinic may need state healthcare permits, a medical director agreement, HIPAA privacy policies, billing setup, and a CLIA waiver if lab testing applies. Cost rises with prescribing, controlled substances, and payer billing, so scope matters before you buy forms or insurance.
Monthly carry
Here’s the quick math: the recurring floor is $4,950 per month from $3,000 vehicle insurance, $1,200 professional liability insurance, and $750 legal and compliance fees. Add malpractice insurance and commercial auto coverage, then size the budget around staffing mix, lab use, and whether billing runs in-house or through a partner.
Scope drivers
One site, one scope, lower cost. A clinic that does only basic primary care needs less setup than one that adds lab draws, point-of-care testing, or controlled substances. Nonprofit, for-profit, and health system partner models also change the compliance load, because billing rules, governance, and insurance needs are not the same.
Risk check
If the clinic uses a mixed staff model, the file set gets bigger fast: credentialing, onboarding, HIPAA training, and billing controls all need to match the services offered. The practical test is simple: every added service, from lab testing to prescribing, should justify its own permit, policy, and insurance line.
Technology, Connectivity, and Billing Infrastructure Startup Expense
Setup Cost
$50,000 covers the one-time tech build: $20,000 for IT infrastructure and $30,000 for EHR implementation. That budget should include scheduling, billing, claims clearinghouse, intake, tablets, laptops, mobile hotspot, telehealth tools, data security, reporting, backup connectivity, and device management.
What It Covers
Size this from device count, setup hours, and install work. The real inputs are how many tablets and laptops you need, whether the clinic must chart offline, and how much backup connectivity rural routes require. If claims are filed the same day, build for faster sync and cleaner handoff.
Count each device.
Test offline charting.
Plan backup signal.
Monthly Load
Recurring cost starts with $1,000 per month for EHR software, plus 2% of Year 1 revenue for EHR and billing transaction fees. One clean way to think about it: the more claims and visits you process, the higher the monthly fee drag.
Go-Live Checks
Test payer mix, offline charting needs, rural connectivity, privacy workflow, and claim submission timing before you buy. If staff must document in dead zones, the system needs stronger sync and backup paths. That keeps billing moving and cuts rework when claims go out.
Staffing Readiness, Launch Preparation, and Operating Reserve Startup Expense
Launch Cash
The launch bridge is the issue, not the steady-state headcount. Year 1 admin wage base is $265,000 per year, or about $22,083 per month, before the first collections land. That cash has to cover recruiting, credentialing, onboarding, training, outreach, and scheduling setup while the clinic builds volume.
Staffing Base
Use this line item for the hiring and setup work that makes service possible. First-year clinical staffing assumes 1 physician, 2 nurse practitioners, 3 medical assistants, 2 phlebotomists, and 2 Driver EMTs. The estimate needs role counts, pay rates, and ramp timing, not just an annual payroll target.
Launch Discipline
Keep launch readiness separate from long-term payroll. Start with credentialing and onboarding before routes expand, then stage training and scheduling so labor matches booked stops. The main mistake is staffing to full-year demand on day one; that burns cash before fee-for-service collections catch up.
Cash Reserve
The operating reserve is a cash bridge, not extra profit. Plan for a minimum $486,000 cash balance by Month 6 so the clinic can pay staff, keep outreach moving, and absorb slow collections without cutting service capacity.
Compare 3 Startup Cost Scenarios
Startup cost scenarios
A mobile clinic gets expensive fast once vehicles, compliance, staff, and cash reserve stack up. Lean, Base, and Full show how service depth changes funding needs and operating risk.
Lean, Base, and Full launch cost comparison
Scenario
Lean LaunchSmall footprint
Base LaunchModel plan
Full LaunchHigher complexity
Launch model
Start with one vehicle, core visits, and a narrow service mix to keep cash needs down.
Run the model as planned with two vehicles, the full core kit, and the Month 6 cash reserve.
Expand service depth, diagnostics, staffing, and reserve to support more sites and more compliance work.
Typical setup
Use lighter equipment, a smaller team, and a leaner compliance stack.
Keep the full equipment and IT stack, plus the staffing plan in the source model.
Add stronger diagnostic coverage, more staff runway, and a larger cash buffer.
Cost drivers
One vehicle
core equipment
small reserve
basic compliance
slim staffing
Two vehicles
vehicle customization
equipment set
IT/EHR
6-month reserve
More diagnostics
larger staffing
extra compliance
bigger reserve
added customization
Planning rangeCAPEX only
Below $580,000Lower cash need
$580,000 - $1,066,000Model baseline
Above $1.1MHigher cash need
Best fit
Best for founders testing demand in one area before adding a second unit.
Best for teams that want the source plan and enough cash to absorb early ramp-up.
Best for operators with secured demand, stronger funding, and a longer launch runway.
!
Planning note: Scenario ranges are planning assumptions from the model, not vendor quotes or fixed bids.
Hold enough reserve to cover the gap before cash receipts stabilize In this plan, the minimum cash need reaches $486,000 in Month 6, while fixed overhead and admin payroll run about $40,833 per month before variable supplies and fuel That reserve is separate from the $580,000 CAPEX budget
Not always, but this researched plan includes two vehicles at $150,000 each A single-vehicle launch may reduce CAPEX, insurance, fuel, and maintenance, but it can also cap service volume and create downtime risk The right count depends on route density, care scope, staffing, and whether missed clinic days would hurt contracts or grants
The best used-vehicle strategy is to price the total clinic-ready unit, not just the vehicle This model budgets $300,000 for two vehicles plus $100,000 for customization, so upfit quality matters Used units can save cash, but maintenance, accessibility, generator capacity, HVAC, plumbing, and clinical layout can erase the headline savings
In this model, breakeven is shown in Month 1, with payback over 26 months That result depends on first-year service volume, including 1 physician, 2 nurse practitioners, 3 medical assistants, 2 phlebotomists, and 2 Driver EMTs If credentialing, route demand, grants, or reimbursement collections slip, cash break-even can move later
Not necessarily A nonprofit may access grants or donated support, but the vehicle, equipment, compliance, insurance, staffing, and technology needs still exist This plan includes $580,000 in CAPEX, $18,750 in monthly fixed overhead, and $265,000 in Year 1 admin wages Funding source changes the cash plan, not the operating reality
About the author
Peter Walsh
Launch Planning Specialist
Peter Walsh is a launch planning specialist at Financial Models Lab who helps online business beginners check whether a business idea is financially realistic by breaking down operating cost estimates into clear, practical planning steps. He focuses on opening and running small businesses, and he explains business costs in a helpful, plain-spoken way without unnecessary jargon.
Choosing a selection results in a full page refresh.