Plastic Surgery Center Startup Costs With $455K Monthly Overhead
You’re budgeting a US plastic surgery center, so the opening plan needs to separate one-time CAPEX, pre-opening expenses, and working capital for the first operating year The model’s known monthly fixed overhead is $45,500 before payroll, with a Month 1 through Month 60 planning period and a Year 1 revenue run-rate of $226,100/month at modeled capacity These figures are researched planning assumptions, not vendor quotes, financing guarantees, or state-specific legal advice
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates the capitalized startup assets needed to open a plastic surgery center, before working capital or payroll runway.
!
What's not included This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, rent deposits, debt service, working capital, launch marketing, insurance premiums, and other operating expenses.
Calculate Fuding Needs
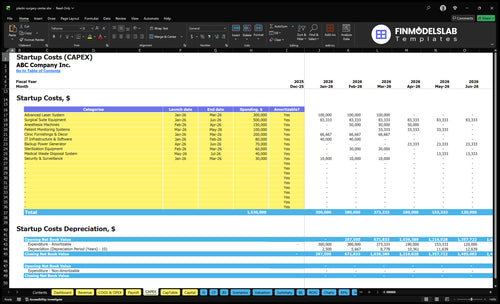
Startup cost summary
This table breaks startup spend into major CAPEX items and the opening cash reserve needed before the clinic stabilizes.
Highlighted CAPEX$1,250,000Base planning example
Excluded cash needs$186,000Outside CAPEX total
Funding need$1,436,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Surgical Suite Equipment
$500,000
Primary operating room buildout and surgical tools
Yes
Advanced Laser System
$300,000
Laser procedure platform and installation
Yes
Clinic Furnishings & Decor
$200,000
Patient-facing space fitout and furnishings
Yes
Anesthesia Machines
$150,000
Anesthesia equipment for surgical cases
Yes
Patient Monitoring Systems
$100,000
Monitoring hardware for procedure and recovery rooms
Yes
Operating Reserve
$186,000
Month 6 cash trough from fixed overhead and payroll ramp
A lean consult-and-minor-procedure setup keeps buildout light, while a full multi-room center needs more rooms, devices, staff, and cash to carry the ramp.
Lean, Base, and Full launch scenarios for a plastic surgery center
Scenario
Lean LaunchLower CAPEX
Base LaunchBalanced launch
Full LaunchMaximum capacity
Launch model
Start with consults and minor procedures, with limited operating-room buildout and a narrow anesthesia, sterilization, and recovery footprint.
Open with the core surgical and non-surgical mix using 2 surgeons, 1 anesthesiologist, 3 nurses, 1 injectable specialist, and 1 laser technician.
Build a multi-room center with more surgeons, more rooms, advanced devices, and a larger cash buffer for the ramp.
Typical setup
Keep one main room, a small team, and only the core devices needed for low-acuity work.
Use the provided opening service mix and a standard clinic layout sized for steady patient flow.
Add higher room count, more support staff, and more equipment for broader aesthetics and surgical volume.
Cost drivers
Reduced room buildout
smaller device set
lighter staffing
less recovery space
Core surgical suite
anesthesia equipment
staffing ramp
sterilization and monitoring
working capital
Extra rooms
advanced devices
larger staffing
stronger working capital
wider recovery capacity
Planning rangeCAPEX only
$900,000 - $1,300,000Lower cash need
$1,500,000 - $2,200,000Core launch band
$2,500,000 - $3,500,000Highest cash need
Best fit
Fits owners testing demand before funding a larger surgical footprint.
Fits operators who want a practical launch with a balanced service mix.
Fits teams aiming for maximum throughput and a broader premium service menu.
!
Planning note: These scenario ranges are researched planning assumptions, not exact quotes or bids.
What hidden costs should a plastic surgery center budget for?
Your CAPEX calculator will miss the cash you need to open and stay open. For a Plastic Surgery Center, budget for malpractice coverage, general liability, accreditation prep, credentialing, compliance consulting, legal formation, policies, inspections, staff training, EMR setup, payment setup, deposits, and launch marketing; read more in How Much Does The Owner Of The Plastic Surgery Center Typically Make? so you also cover operating cash. Hidden overhead is already about $45,500/month before payroll, with $3,000 legal and accounting, $1,500 IT, $1,800 cleaning and maintenance, $1,200 security, and $500 office supplies. Year 1 variable costs can also run hot: 70% medical supplies and injectables, 15% pharmaceuticals, 50% marketing and advertising, and 25% payment processing fees.
Upfront cash needs
Pay malpractice and liability coverage
Fund accreditation and credentialing
Cover legal formation and policies
Pay deposits and launch marketing
Run-rate costs
Budget $45,500/month before payroll
Carry several months of payroll and rent
Expect 70% supplies and injectables
Plan for 25% payment fees
What are the biggest costs in opening a plastic surgery center?
The biggest costs in a Plastic Surgery Center are the surgical-ready buildout, medical equipment, accreditation and insurance, and clinical payroll. An office-only aesthetics model is much cheaper; once you add anesthesia, sterilization, recovery, HVAC, plumbing, electrical, and code compliance, the spend jumps fast. Here’s the quick math: visible fixed costs already show $25,000/month for the facility lease and $10,000/month for insurance and accreditation, before staff and equipment.
Big cost drivers
Surgical buildout costs more than office space
Medical equipment adds major upfront spend
HVAC and plumbing need clinical specs
Code compliance drives hidden upgrades
Year 1 payroll load
Medical Director: $350,000/year
Lead Surgeon: $300,000/year
Anesthesiologist: $250,000/year
3 RNs: $240,000/year total
The visible Year 1 salary lines total $1,435,000, or about $119,583/month, before taxes and benefits. Add the Injectable Specialist at $120,000, the Laser Technician at $75,000, and the Practice Manager at $100,000, and labor stays the main pressure point.
How should founders fund a plastic surgery center?
For a Plastic Surgery Center, fund the launch in four buckets: CAPEX, pre-opening expenses, working capital, and the cash gap. Build the model for Month 1 through Month 60, and tie hiring, accreditation, and revenue ramp to real start dates so the funding ask matches the launch plan. The next step is cost sizing, then run downside cases before you choose financing.
Use-of-funds plan
CAPEX goes on a separate tab.
Startup expenses sit outside CAPEX.
Working capital covers the early cash gap.
Keep payroll timing in the model.
Ramp and assumptions
Model Year 1 to Year 5 capacity ramps.
Surgeons move from 500% to 750%.
Injectable specialists move from 600% to 850%.
Show fixed, variable, and depreciation costs.
Key Takeaways
Facility buildout is major CAPEX, not office overhead.
Equipment quotes must match your onsite procedure mix.
Licensing costs split into setup, recurring, and deposits.
Staffing and launch cash can outrun pre-revenue reserves.
Plastic Surgery Center Core Five Startup Costs
Facility Buildout Startup Expense
Buildout Scope
This is major CAPEX, not office fit-out. It covers reception, consult rooms, procedure rooms, surgical areas, recovery space, sterilization flow, medical gas or anesthesia support if needed, HVAC, plumbing, electrical, accessibility, and code compliance. There’s no square footage or unit cost in the source, so don’t price it yet.
What To Price
Start with the inputs that change the build: facility size, lease condition, procedure scope, number of rooms, and accreditation target. Then get contractor, engineer, and equipment vendor quotes. If the center will do only consults and injectables, the build is very different from an operating-room-level setup.
Facility size
Room count
Procedure mix
Accreditation target
How To Control It
Don’t treat this like a normal office buildout. The biggest savings come from matching the space to the actual procedure mix, not overbuilding for future maybe-work. Protect sterilization, ADA access, HVAC, and electrical capacity. Use phased finishes only where they don’t affect patient flow or compliance.
Match rooms to demand
Phase noncritical finishes
Keep code items intact
Lease And Cash Pressure
With a $25,000/month lease anchor and $45,500/month fixed overhead before payroll, buildout timing matters. If lease payments start before the space is ready, you burn cash fast. Don’t publish a buildout CAPEX range until you have quotes and the lease terms that define who pays for tenant improvements.
Medical Equipment Startup Expense
Buildout Plan
Buildout is major CAPEX, not office setup. It covers reception, consult rooms, procedure rooms, surgical areas, recovery, sterilization flow, HVAC, plumbing, electrical, accessibility, and code work. Price it from contractor quotes after you lock facility size, lease condition, room count, procedure scope, and accreditation target; the $25,000/month lease and $45,500/month fixed overhead sit on top.
Which procedures happen onsite?
Do OR-level standards apply?
How many rooms are needed?
Equipment Quote List
Quote the opening kit by procedure, not by guess. Map surgical and non-surgical needs to the team mix: surgeons, anesthesiologists, nurses, injectable specialists, and laser technicians. Include surgical tables, lights, monitors, anesthesia gear, sterilizers, instruments, recovery equipment, exam room gear, injectables storage, and photo systems; keep lasers and energy devices in a separate premium quote file.
Use vendor quote fields only.
Separate required and premium devices.
Track install and maintenance too.
Compliance Stack
Split this into one-time filings, recurring subscriptions, and deposit-based work. Cover state facility rules, physician licensing, ambulatory surgery accreditation if needed, CLIA steps if relevant, HIPAA, formation, contracts, policies, credentialing, inspections, and compliance consulting. Confirm requirements before signing a lease or buying equipment; $10,000/month insurance and accreditation plus $3,000/month legal and accounting are recurring anchors.
Staffing Runway
Staffing readiness is pre-open working capital, not CAPEX. The opening mix is 2 surgeons, 1 anesthesiologist, 3 nurses, 1 injectable specialist, and 1 laser technician. Build payroll, credentialing, and training into the runway before revenue starts; Year 1 salary lines include $350,000 for a medical director, $300,000 for a lead surgeon, and $250,000 for anesthesia.
Launch Cash
Bundle software, supplies, insurance, and launch spend into the first cash draw. Recurring anchors are $1,500/month for IT and software, $10,000/month for insurance and accreditation, and 50% of Year 1 revenue for marketing. Initial medical supplies and injectables run at 70% of revenue, with pharmaceuticals at 15%.
Licensing And Compliance Startup Expense
State Rules
Licensing starts with state facility rules, physician licenses, and any ambulatory surgery accreditation tied to your procedures. If you run lab testing, check CLIA (Clinical Laboratory Improvement Amendments); if you handle patient data, build HIPAA policies. This is mostly planning work, and the cost mix changes by state, ownership model, and scope.
Setup Costs
One-time setup usually covers legal formation, contracts, policies, credentialing, and inspection prep. Ongoing burden is clearer: $10,000/month for insurance and accreditation plus $3,000/month for legal and accounting, before payroll. If filings or surveys need deposits, track them separately so startup cash does not hide inside monthly run rate.
One-time: formation and policies
Monthly: insurance and legal
Deposits: filings and surveys
Before Lease
Do the compliance check before you sign a lease or buy equipment. The safest savings come from matching approvals to the exact procedure mix, since a surgical center, office-based clinic, and lab-backed practice do not face the same rules. Early review cuts rework, duplicate filings, and wasted buildout spend.
Run-Rate Impact
This line is not small. The source fixed load already includes $10,000/month for insurance and accreditation and $3,000/month for legal and accounting, inside $45,500/month of fixed overhead before payroll. If the lease adds $25,000/month, founders need the compliance budget locked before opening day.
Staffing Readiness Startup Expense
Pre-Opening Payroll
Staffing readiness is cash, not CAPEX. For this opening mix, the visible Year 1 salary lines total $1.435M: $350k medical director, $300k lead surgeon, $250k anesthesiologist, $240k for 3 RNs, $120k injectable specialist, $75k laser technician, and $100k practice manager if FTE is confirmed.
How To Budget
Estimate it as role count × monthly salary × months before revenue. For this center, plan around 2 surgeons, 1 anesthesiologist, 3 nurses, 1 injectable specialist, and 1 laser technician, plus training, credentialing, front desk, and billing support. Use the visible salary lines as the base case, then add open roles only after FTEs are signed.
Use start dates, not guesses
Separate paid training time
Confirm FTE before budgeting
Control The Burn
Keep nonclinical hires tied to opening dates and credentialing milestones. The $100k practice manager line stays pending until FTE is confirmed, so don’t lock it into the base case. What this hides: recruiting delays can turn a clean salary plan into idle payroll.
Stage hires by room opening
Track credentialing weekly
Avoid full-time overlap
Cash Buffer
This is working capital, so it hits cash before first procedure revenue. It also sits on top of the $45,500 monthly fixed overhead before payroll, so timing matters more than the title on the org chart.
Technology, Supplies, Insurance, And Launch Startup Expense
Buildout
Reception, consult rooms, procedure rooms, surgical areas, recovery, sterilization flow, medical gas or anesthesia support, HVAC, plumbing, electrical, access, and code compliance are major CAPEX. Size the quote by lease condition, facility size, room count, procedure scope, and accreditation target. With a $25,000/month lease anchor and $45,500/month fixed overhead before payroll, this needs a vendor quote, not a guess.
Equipment
List surgical tables, lights, monitors, anesthesia gear, sterilizers, instruments, recovery equipment, exam room gear, injectables storage, lasers, and photography systems. Split must-have opening items from optional premium devices. Estimate with quotes by unit count, room count, and which procedures run onsite. The mix of surgeons, anesthesiologists, nurses, injectable specialists, and laser techs should match the equipment list.
Compliance
Use one-time setup, monthly recurring, and deposit buckets for state rules, licensing, accreditation, Health Insurance Portability and Accountability Act (HIPAA) compliance, formation, contracts, policies, credentialing, inspections, and consulting. Recurring anchors are $10,000/month for insurance and accreditation and $3,000/month for legal and accounting. Confirm facility and scope rules before signing the lease or buying equipment.
Launch Cash
Cover electronic medical record (EMR), practice management, payments, website, booking, photography, initial supplies, surgical disposables, injectables, malpractice/general liability, marketing, and deposits. Separate setup fees and prepaid premiums from recurring spend: $1,500/month IT and software, $10,000/month insurance and accreditation, and 50% of Year-1 revenue for marketing. The first-month recurring floor is $11,500 before payroll and rent. Supplies tie to 70% of revenue for inventory and injectables plus 15% for pharmaceuticals.