Preoperative Assessment Clinic Startup Costs: $287K CAPEX Plan
You’re funding the clinic before reimbursements and referral volume settle, so the opening budget needs more than equipment The first operating year model includes $287,000 in scheduled CAPEX and a $886,000 Month 1 minimum cash need These are planning assumptions for launch funding, not vendor quotes or guaranteed operating results
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates the capitalized startup assets needed to open a preoperative assessment clinic, including fit-out, equipment, IT, furniture, signage, and contingency.
!
What this excludes This only covers capitalized startup assets. It excludes payroll runway, working capital, rent deposits, debt service, inventory, payer delays, and ongoing operating expenses.
Calculate Fuding Needs
Startup cost summary
This table shows the main opening assets and the non-CAPEX cash reserve needed to launch the clinic.
Highlighted CAPEX$240,000Base planning example
Excluded cash needs$886,000Outside CAPEX total
Funding need$1,126,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Medical Examination Equipment
$75,000
Exam tables, diagnostic tools, and procedure setup
Yes
Waiting Area Renovation
$60,000
Buildout scope, finishes, and patient flow changes
Yes
EHR Implementation and Setup
$45,000
System setup, data migration, and implementation work
Yes
Clinic Office Furniture
$35,000
Desks, chairs, storage, and front-desk layout
Yes
EKG Machines and Monitors
$25,000
Cardiac screening equipment and monitoring devices
Yes
Opening cash reserve
$886,000
Month 1 minimum cash need for payroll and operating runway
No
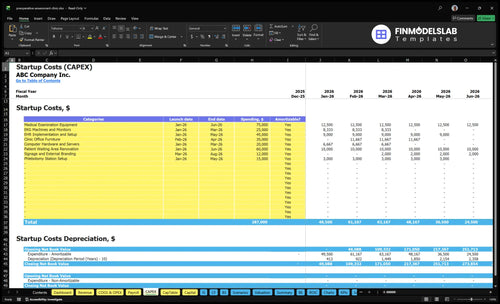
What does the CAPEX tab show?
Preoperative Assessment Clinic Financial Model Template CAPEX tab maps $287k, Month 1-8 timing, depreciation/amortization, and $886k cash; validate payer timing.
Screenshot highlights
Year 1 revenue $4.457m
Fixed costs $23,750 monthly
Variable costs 18.5%
Compare 3 Startup Cost Scenarios
Startup cost scenarios
Startup costs swing with how much testing you do on site, how ready the staff is, and how deep the clinic's systems go. Referral volume, payer mix, and credentialing timing drive the right launch size.
Lean, Base, and Full launch paths for a preoperative assessment clinic.
Scenario
Lean LaunchLower CAPEX
Base LaunchBalanced launch
Full LaunchHigher scope
Launch model
Start with referral-based evaluations and a limited onsite test menu.
Build a standard clinic around the source CAPEX of $287,000 and the Month 1 minimum cash need of $886,000.
Add broader onsite testing, more exam rooms, and heavier integrations from day one.
Typical setup
Use fewer rooms, basic equipment, and lighter technology integration.
Use the modeled core equipment, standard rooms, and normal staffing and systems.
Use deeper compliance support, stronger systems, and more working capital for ramp-up.
Cost drivers
Limited diagnostics
fewer exam rooms
basic EHR setup
smaller staff
lighter compliance support
Source CAPEX
core medical equipment
EHR implementation
lease and build-out
working capital
Broader testing
more exam rooms
heavier integrations
compliance support
deeper working capital
Planning rangeCAPEX only
$650,000 - $900,000Lower funding need
$886,000 - $1,173,000Core model
$1,150,000 - $1,500,000Higher funding need
Best fit
Best for clinics with steady referrals, slow credentialing, and a narrow service mix.
Best for teams with a solid referral pipeline and moderate payer and credentialing risk.
Best for operators with strong referrals, faster credentialing, and a payer mix that supports more onsite work.
!
Planning note: These scenario ranges are researched planning assumptions, not exact quotes or bids.
What are the biggest startup costs for a preoperative assessment clinic?
For a Preoperative Assessment Clinic, the biggest startup costs are the physical buildout and clinical gear: $60,000 for the waiting area plus leasehold work, $75,000 for medical exam equipment, $25,000 for EKG machines and monitors, $15,000 for phlebotomy setup, $45,000 for EHR implementation, and $20,000 for hardware. That puts hard startup spend at about $240,000 before staffing and compliance. One line: the room, the machines, and the system cost more than the first few hires.
Facility and equipment
$60,000 waiting-area renovation
Reception, exam, and consult rooms
ADA access, plumbing, electrical, HVAC
EKG, phlebotomy, and exam gear
Staffing and compliance
Credentialing and onboarding
Protocol training before opening
Pre-opening payroll during ramp-up
HIPAA, OSHA, and payer enrollment support
What hidden costs come with starting a preoperative assessment clinic?
The biggest hidden cost is cash, not the exam room. A Preoperative Assessment Clinic can face a $12,500 monthly lease deposit, plus $23,750 in fixed monthly commitments before wages, so the business burns money early even before the first patient is seen. For a deeper cost lens, see How Increase Profits Preoperative Assessment Clinic? Also, Year 1 variable costs can run at 185% of base activity from supplies, lab processing, commissions, and EHR fees, which makes reimbursement timing a real runway risk.
Upfront costs
Lease deposit on $12,500 rent
Insurance setup before care starts
Malpractice coverage before launch
Payer enrollment and credentialing delays
Run-rate risks
Training and policy writing time
Medical waste and cybersecurity setup
Marketing spend before revenue lands
Lab and EHR fees hit cash fast
How should you plan funding for a preoperative assessment clinic?
Plan the funding in four buckets: $287,000 of CAPEX, pre-opening expenses, operating runway, and a payer timing reserve. The Month 1 minimum cash need is $886,000, and CAPEX should run from Month 1 through Month 8 because signage stretches to Month 8 while clinical assets land in Months 3 to 6. Use a Year 1 revenue case of $4.457 million at 55% to 65% capacity, but don’t assume Month 1 breakeven is guaranteed.
Funding buckets
$287,000 CAPEX schedule
Pre-opening expenses
Operating runway
Payer timing reserve
Risk checks
Slow credentialing
Lower utilization
Delayed referrals
Higher build-out cost
Key Takeaways
Landlord work should stay separate from founder build-out.
Medical equipment starts around $115,000 before supplies.
EHR setup adds $65,000 plus monthly IT fees.
Pre-opening payroll is separate from ongoing staffing costs.
Preoperative Assessment Clinic Core Five Startup Costs
A clinic build-out needs reception, waiting, exam rooms, consultation rooms, specimen collection, staff work areas, secure records, ADA access, HVAC, plumbing, electrical, signage, and a contractor contingency. Use $60,000 for patient waiting area renovation and $12,000 for signage and external branding as base CAPEX anchors.
Budget inputs
Estimate this cost from square footage, local construction rates, landlord allowance, plumbing needs, and whether medical gas is required. Here’s the quick math: if the space already has exam-room shell work, some leasehold improvements sit outside listed CAPEX; if not, founder-funded build-out rises fast.
Get two contractor quotes
Confirm landlord allowance early
Test inspection timing risk
Spend control
Keep landlord-paid work separate from founder-funded work, or the budget gets messy fast. Push for the landlord to cover base shell items, then fund only clinic-specific items like signage, waiting area finish-out, and room fit-out. The main swing factor is whether exam-room construction is already in place.
Scope by room, not by guess
Reserve contingency for delays
Track landlord invoices separately
Cost split
What this estimate hides is timing risk: HVAC, plumbing, electrical, and inspections can move the number as much as the room count. If the site needs new exam-room construction, broader leasehold improvements may sit outside the listed CAPEX, so separate landlord-paid shell work from founder-funded clinic fit-out before signing.
Compliance And Insurance Costs For A Preoperative Assessment Clinic Startup Expense
What It Covers
This cost covers entity formation, state medical practice rules, professional licenses, provider credentialing, payer enrollment, CLIA waiver if waived testing is offered, OSHA and HIPAA policies, consent forms, referral contracts, billing compliance, malpractice coverage, general liability, workers’ compensation if needed, and insurance binders. The fixed anchor here is $1,800 per month for general liability insurance.
What Drives Price
Budget from the clinic’s ownership structure, onsite testing scope, payer mix, supervising physician rules, and whether billing runs directly or through affiliated providers. Add carrier quotes for malpractice and workers’ compensation, plus time for credentialing and enrollment. State licensing fees vary, so use local rules instead of a universal figure.
How To Control It
Keep the scope tight: use referral-out testing unless onsite labs truly add value, and limit payer enrollment to plans you can serve well. Do not cut HIPAA or OSHA work; rework costs more later. One clean move is separating landlord-paid work from founder-funded compliance so cash needs stay real.
Insurance Binders
Ask for insurance binders early, since landlords and hospital partners often want proof before move-in. Carry malpractice, general liability, and workers’ compensation if staff exposure applies. The monthly insurance line is only part of the spend; timing, claims history, clinical scope, and specimen testing all move the price.
Preoperative Assessment Clinic Medical Equipment Startup Expense
Core gear
The main equipment budget starts with $75,000 for medical examination equipment, $25,000 for EKG machines and monitors, and $15,000 for phlebotomy station setup. That covers exam tables, vital-sign monitors, scales, specimen handling, crash cart readiness, and storage. Add point-of-care testing only if the clinic will actually run it onsite.
What to buy
Price the build by workflow, not by guesswork. Use vendor quotes for each unit, then separate exam-room gear, EKG gear, and blood-draw supplies. The key question is simple: does the clinic test onsite, or send work out?
Count exam rooms first
Quote each device separately
Keep backup supplies on hand
Where to save
Do not buy extra diagnostics for low volume. If testing is referred out, keep the equipment set lean and avoid idle gear. Here’s the quick math: onsite scope drives CAPEX, while disposable clinical supplies run at 45% of revenue and diagnostic lab processing fees at 65% of revenue as operating costs, not startup cost.
Scope drives spend
If the clinic offers more onsite diagnostics, cash goes into EKGs, monitors, phlebotomy setup, specimen handling, and testing storage. If it mostly refers out, the startup bill stays closer to exam-room basics and the lab cost moves into monthly operating spend instead.
EHR And IT Costs For A Preoperative Assessment Clinic Startup Expense
Core IT Spend
For a preoperative assessment clinic, the first IT check is about $65,000 in CAPEX: $45,000 for EHR implementation and setup plus $20,000 for computers, hardware, and servers. Then budget $2,200 a month for IT maintenance and cybersecurity, plus EHR transactional fees at 25% of Year 1 revenue.
What It Covers
This spend covers the EHR, practice management, scheduling, billing, patient portal, secure messaging, e-prescribing, eligibility checks, networking, backup, and interfaces with surgeons, hospitals, labs, and billing workflows. Interoperability means systems share patient data without manual re-entry. The big inputs are implementation, data migration, training, interface work, and cybersecurity requirements.
Price each interface separately
Scope migration before go-live
Confirm backup and recovery terms
Control The Cost
Keep the first build tight. Start with the modules you need on day one, then phase extra integrations after launch. Don’t cut cybersecurity or data backup to save a little cash. The cheapest mistake is usually scope control; the expensive mistake is paying twice for cleanup, re-entry, or failed interfaces.
Launch core workflows first
Delay nonessential integrations
Train staff before go-live
Budgeting Trap
The hidden pressure is variable cost. With EHR transaction fees set at 25% of Year 1 revenue, the monthly bill moves with volume, not just with headcount. So the budget should track collections, claim flow, and interface volume, not only the one-time setup quote and server purchase.
Pre-Opening Staffing Costs For A Preoperative Assessment Clinic Startup Expense
Launch Hiring
Pre-opening hiring covers recruiting, background checks, credentialing, payer enrollment paperwork, onboarding, protocol training, scheduling templates, care pathways, emergency procedures, and billing workflows. Treat it as one-time launch payroll, not monthly burn. Year 1 service staffing assumes 2 perioperative physicians, 3 nurse practitioners, 2 physician assistants, 4 registered nurses, and 4 medical assistants.
Admin Payroll
Administrative payroll should be tracked separately from clinical staffing. The plan includes a $280,000 medical director, $95,000 clinic administrator, $85,000 sales and relations manager, 2 patient coordinators at $55,000 each, 1 billing and coding specialist at $65,000, and 2 receptionists at $42,000 each. That totals about $59,900/month before taxes and benefits.
Ramp Control
Keep pre-open spend lean by hiring in waves, finishing credentialing before start dates, and using draft workflows early so staff train once. Common mistake: putting every role on payroll before payer enrollment and schedule demand are ready. One clean rule: open with the smallest team that can safely run the first clinic days.
Cash Plan
The budget test is simple: if pre-opening payroll runs for 2 to 3 months, use the monthly admin base of $59,900 plus the clinical ramp team, then add employer taxes and benefits on top. Separate founder-funded launch payroll from ongoing operating payroll so setup cash does not blur into steady-state staffing.