Pulmonary Function Testing Center Startup Costs: $263K CAPEX Plan
A US pulmonary function testing center in this model needs at least $263,000 of identified startup CAPEX before reserves That includes $108,000 for testing equipment, $120,000 for clinic buildout, and $35,000 for medical-grade IT infrastructure Total funding need is higher once you add pre-opening costs, rent deposits, insurance, payroll readiness, payer enrollment, and working capital As a researched planning assumption, one month of known fixed overhead plus listed non-clinical payroll is about $50,200, while three months is about $150,700, before technologist wages
Calculate Fuding Needs
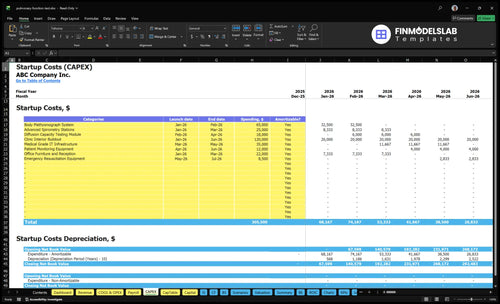
Startup cost summary
Shows startup spending for clinic buildout, testing equipment, IT, and opening cash needs for the pulmonary function testing center.
Highlighted CAPEX$267,000Base planning example
Excluded cash needs$837,000Outside CAPEX total
Funding need$1,104,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinic Interior Buildout
$120,000
Main clinic buildout work
Yes
Body Plethysmograph System
$65,000
Core lung-function testing hardware
Yes
Medical-Grade IT Infrastructure
$35,000
Medical records and network setup
Yes
Advanced Spirometry Stations
$25,000
Spirometry testing rooms
Yes
Office Furniture and Reception
$22,000
Patient check-in and waiting area fit-out
Yes
Operating Reserve
$837,000
Minimum cash at Month 2 plus opening loss coverage
No
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets only for a pulmonary function testing center launch.
!
CAPEX only This tool covers capitalized startup assets only. It excludes payroll runway, inventory, rent deposits, debt service, working capital, reimbursement delays, marketing, and other operating expenses.
Costs swing fast here because equipment, buildout, staffing, and reserve cash all move together. Lean cuts scope, Base matches the model, and Full adds rooms, staff, and deeper coverage.
Lean, Base, and Full launch funding needs.
Scenario
Lean LaunchDeferred scope
Base LaunchModel anchor
Full LaunchHigher scale
Launch model
Start with spirometry-first testing and defer higher-scope modules.
Open with the modeled multi-test clinic and Year 1 staffing plan.
Add more rooms, more staff, and reserve cash from day one.
Typical setup
Use a smaller test menu, lighter buildout, and a lean reserve while referrals ramp.
Use the $263,000 CAPEX anchor, body plethysmography, and the full Year 1 team.
Use deeper equipment coverage, higher testing capacity, and a larger operating cushion.
Cost drivers
Deferred plethysmograph
smaller buildout
lighter IT
fewer reserve months
Body plethysmograph ($65,000)
clinic buildout ($120,000)
medical IT ($35,000)
monthly overhead ($19,550)
Year 1 staffing
Extra rooms
expanded equipment
added staff
reserve months
bigger buildout
Planning rangeCAPEX only
$650,000 - $775,000Smallest cash need
$800,000 - $900,000Model cash band
$950,000 - $1,150,000Highest cash need
Best fit
Best for a thin referral base and limited funding cushion.
Best for a steady referral base and payer setup that can support a full diagnostic menu.
Best for strong referrals, payer readiness, and a larger capacity plan.
!
Planning note: These ranges are researched planning assumptions for launch modeling, not vendor quotes or live bids.
How much money do you need to open a pulmonary function testing center?
You need at least $263,000 in identified capital expenses (CAPEX) to open a Pulmonary Function Testing Center: $108,000 diagnostic equipment + $120,000 buildout + $35,000 IT. For a funded launch, plan $313,200 with one month of known overhead or $413,700 with three months; this How To Launch Pulmonary Function Testing Center? gap matters because startup cost isn’t the same as total funding need.
Bare Minimum
$108,000 diagnostic equipment
$120,000 clinic buildout
$35,000 IT setup
$263,000 opening CAPEX
Funded Launch
$50,200 one-month overhead reserve
$150,700 three-month overhead reserve
Excludes technologist wage cushion
Plan around $161,760 modeled monthly revenue
What hidden costs do founders miss when opening a pulmonary function testing center?
If you open a Pulmonary Function Testing Center, the hidden costs are the setup items before day one and the cash gap after launch. The listed recurring costs alone total $16,150 a month: $12,500 lease, $1,500 liability insurance, $1,200 EHR and practice management software, and $950 utilities and biohazard waste. For the operating side, use What 5 KPIs Should Pulmonary Function Testing Center Track? and treat reimbursement delays as working capital, not CAPEX.
Before opening
Lease deposits come first.
Payer enrollment and credentialing take time.
Medicare setup, legal, and accounting add cost.
Training, website, and launch marketing need cash.
Monthly burn
Facility lease: $12,500.
Professional liability: $1,500.
Software: $1,200.
Utilities and waste: $950.
How much does pulmonary function testing equipment cost?
For a Pulmonary Function Testing Center, a full starter setup is about $108,000 before calibration syringes, testing gas, filters, mouthpieces, carts, computer interfaces, installation, warranties, and service contracts. A spirometry-only launch costs less, and ongoing equipment maintenance is modeled at $2,800 per month after opening.
Core equipment cost
$65,000 body plethysmograph system
$25,000 advanced spirometry stations
$18,000 diffusion capacity testing module
Full stack totals $108,000
Budget extras
Calibration syringes and testing gas
Filters, mouthpieces, and carts
Computer interfaces and installation
Warranties, service contracts, $2,800/month maintenance
Key Takeaways
Equipment is the biggest CAPEX driver at $108,000.
Buildout runs months 1 through 6, costing $120,000.
Software starts in Month 3, plus 40% billing fees.
Staffing includes $30,667 monthly nonclinical payroll before technologists.
Pulmonary Function Testing Center Core Five Startup Costs
Pulmonary Function Testing Equipment Startup Expense
Core test lab gear
The modeled equipment CAPEX is $108,000 for a full pulmonary function setup: $65,000 body plethysmograph system, $25,000 advanced spirometry stations, and $18,000 diffusion capacity module. That scope supports spirometry, lung volumes, and diffusion capacity, so match the build to the tests you’ll actually sell.
What the budget includes
Budget for more than the machines. The model also assumes calibration syringe, testing gas, disposable filters, mouthpieces, carts, interfaces, installation, warranty, and service agreements. Here’s the quick math: equipment quote plus setup items and vendor support. Don’t treat the $108,000 as a turnkey ceiling if your site needs extra installation or service coverage.
Ask for itemized vendor quotes.
Separate install from hardware.
Map each device to a service.
Keep the scope tight
Do not buy the full lab if your first referral base only needs spirometry. Start with the tests you can fill, then add lung volumes or diffusion capacity when volume supports it. Year 1 COGS in the model is 65% disposable medical supplies and 35% testing gas and calibration kits, so recurring supply spend starts early.
Buy for booked demand.
Track consumables by test type.
Renew service terms yearly.
Year 1 cost pressure
What this estimate hides is the ongoing burn. Disposable medical supplies make up 65% of Year 1 COGS, with 35% tied to testing gas and calibration kits, so utilization matters fast. If test volume stays low, supply waste and service contracts can make the equipment spend feel heavier than the headline $108,000.
Pulmonary Function Testing Center Staffing and Launch Startup Expense
Launch payroll
The biggest startup burn is people. Year 1 assumes 2 senior pulmonary technologists, 1 junior pulmonary technologist, 1 respiratory therapist specialist, 0 clinical exercise physiologists, and 1 testing assistant, plus non-clinical payroll of about $30,667 per month before technologist wages. That cost starts before steady patient volume does.
Startup spend
This bucket covers recruiting, onboarding, training, pre-opening payroll, uniforms, scheduling protocols, referral outreach, launch supplies, and early local marketing. Estimate it with headcount, months of coverage, vendor quotes, and campaign spend. Keep it separate from monthly payroll so one-time opening costs do not get mixed into ongoing operating burn.
Price each hire by role
Quote training and uniforms
Split launch and monthly costs
Keep costs clean
Start with only the roles needed on day one, then add support as referral volume builds. The clean rule is simple: one-time launch spend in one bucket, recurring wages and supplies in another. That keeps hiring tied to patient flow, not guesswork or a too-early payroll load.
Open with required staff only
Track referral outreach results
Use a live scheduling protocol
Budget floor
The model’s non-clinical payroll floor is about $30,667 per month before technologist wages, so this line is already meaningful before the clinic opens. Add launch-only items on top, then watch supply burn and payroll together once testing starts.
PFT Clinic Licensing, Credentialing, and Insurance Startup Expense
Licensing Scope
This bucket covers the legal base for opening a PFT clinic: entity formation, state and local permits, medical director agreements, payer enrollment, Medicare setup, and a CLIA (Clinical Laboratory Improvement Amendments) applicability review. Keep one-time setup costs separate from monthly insurance and compliance admin, because the right path depends on your services and state rules.
Cost Inputs
Price this from attorney and accountant quotes, filing fees, enrollment work, and the number of policies and workflows you need. Include malpractice insurance, general liability, legal fees, accounting setup, compliance policies, and documentation workflows. The model carries $1,500 per month for professional liability insurance, which sits outside one-time launch costs.
Quote each filing and agreement.
Split setup from monthly burn.
Track payer and Medicare work.
Keep It Tight
Use one healthcare attorney and one credentialing specialist, then get every jurisdictional rule in writing before you spend. That cuts rework on permits, payer enrollment, and CLIA assumptions. Don’t bundle monthly insurance with launch costs; clean separation makes runway math honest and shows what can wait.
Verify scope before filing.
Price monthly coverage separately.
Avoid bad CLIA assumptions.
Check Rules First
If the clinic’s service mix changes, the permit path and CLIA review can change too. Before you file or sign, verify requirements with healthcare counsel and credentialing specialists so you don’t pay for the wrong setup or delay cash collection.
PFT Clinic Buildout Startup Expense
Clinic Buildout
Model this as $120,000 of facility CAPEX, separate from the $12,500 monthly lease. It covers test rooms, reception, patient flow, ADA access review, electrical and data drops, HVAC comfort, infection-control finishes, signage, and waiting furniture. Buildout runs from Month 1 to Month 6, so cash use is phased, not all paid on day one.
What It Covers
Estimate it from contractor quotes, landlord allowance offsets, and the final room plan. The key inputs are suite condition, landlord work letter, and any specialty ventilation needs. If the space is already close to medical use, the budget can stay near plan; if not, tenant improvements and compliance work push it up fast.
Control The Spend
Keep costs down by reusing what already works and locking scope before work starts. Don’t fold lease payments into CAPEX, and don’t skip the ADA or airflow review to save a little upfront. The cleanest control is a fixed quote with clear allowances, so change orders don’t eat the budget mid-build.
Budget Fit
This line belongs in startup budget planning, not monthly overhead. It sits next to equipment, software, licensing, and launch payroll, but it should stay separate in the model so you can see cash needed before opening. One line item, one job: get the clinic ready for testing.
PFT Clinic Software and Billing Startup Expense
IT Stack
The clinic’s software and billing stack covers EHR, practice management, clearinghouse setup, reporting, cybersecurity, computers, phones, website, payment tools, and data connections. The model funds $35,000 of medical-grade IT in Month 3 to Month 5, then $1,200 per month after opening. That is the core operating layer, not a one-time buy.
Estimate It
Build the cost from vendor quotes, device count, setup fees, and months of coverage. The big variable is billing: Year 1 claims and processing are modeled at 40% of revenue, so every software choice should improve clean claims, referral reporting, payer enrollment, and reimbursement lag. Here’s the quick math: more denials mean slower cash.
Trim Waste
Keep the stack lean by choosing tools that talk to each other on day one, since duplicate logins and manual re-entry slow billing and raise errors. Avoid overbuying reports you will not use. The main savings come from tighter claim flow and fewer fixes, not from cutting core security or data links. Clean claims beat cheap software.
Cash Timing
This cost hits cash twice: the $35,000 build lands before launch, and the $1,200 monthly software bill starts after opening while the 40% Year 1 billing fee can delay collections. If payer setup or claim edits take longer, reimbursement lag grows, so the system should support fast enrollment and error checks.