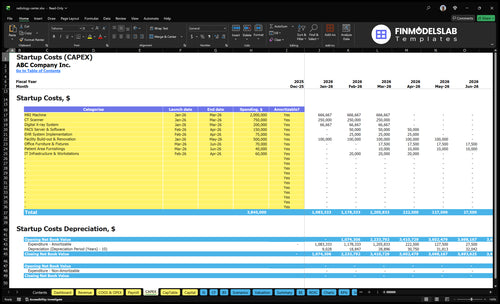
Radiology Center Startup Costs: $385M CAPEX Planning Guide
It costs about $3845M in researched CAPEX to open this radiology center before working capital and financing reserves The largest startup costs are the $20M MRI machine, $750k CT scanner, $500k facility buildout, $200k digital X-ray system, and $285k in PACS, EHR, and IT infrastructure The model also shows a Month 5 minimum cash position of -$2572M, so total funding needs should cover launch timing, payroll, rent, insurance, billing delays, and reimbursement ramp Actual diagnostic imaging center startup costs vary by modality mix, equipment condition, lease terms, accreditation path, and local construction requirements
Calculate Fuding Needs
Startup Cost Summary
Shows startup CAPEX, launch operating costs, and excluded cash needs for a radiology center across low, base, and high scenarios.
Highlighted CAPEX$3,600,000Base planning example
Excluded cash needs$2,572,000Outside CAPEX total
Funding need$6,172,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
MRI Machine
$2,000,000
MRI system size, specs, and installation scope
Yes
CT Scanner
$750,000
Scanner model, service package, and installation
Yes
Facility Build-out & Renovation
$500,000
Leasehold improvements and imaging room build-out
Yes
Digital X-ray System
$200,000
Digital panel specs and room integration
Yes
PACS Server & Software
$150,000
Image archive size, licenses, and integration
Yes
Operating Cash Reserve
$2,572,000
Month 5 cash trough plus launch payroll and fixed costs
No
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates the capitalized startup assets to open a radiology center, including imaging systems, software, build-out, and furnishings.
!
CAPEX only Excludes inventory, payroll runway, deposits, debt service, working capital, licensing, and launch marketing. This calculator covers capitalized startup assets only.
What does the CAPEX tab show?
This screenshot shows the CAPEX tab, with startup costs, launch timing, and depreciation or amortization. Open the Radiology Center Financial Model Template and test assumptions.
CAPEX tab highlights
MRI, CT, X-ray
Buildout and furnishings
Month 1 to 6
Compare 3 Startup Cost Scenarios
Scenario Table
Startup cost moves with scanner count, buildout size, staffing depth, and IT scope. Lean keeps cash use lighter, while Full Launch needs more rooms, people, and working capital.
Lean, Base, and Full launch cost bands for a radiology center.
Scenario
Lean LaunchLowest upfront cash
Base LaunchBalanced launch
Full LaunchMulti-modality hub
Launch model
Start with fewer modalities, fewer scanners, and lean staffing to keep cash use tight.
Launch the core mix with one MRI, one CT, and one X-ray system plus standard staffing.
Build a multi-modality referral hub with more scanner capacity, deeper staffing, and broader IT links.
Typical setup
Use a smaller buildout, limited support staff, and a shorter runway while demand proves out.
This matches the researched model at $3,845,000 CAPEX and a Month 5 cash trough of -$2.572M.
Add more rooms, longer accreditation prep, and a larger cash buffer for a heavier open.
Cost drivers
Fewer modalities
smaller scanner count
lighter buildout
lean staffing
shorter runway
MRI machine
CT scanner
X-ray system
buildout
IT/software
More rooms
extra scanner capacity
deeper staffing
integrated IT
working capital buffer
Planning rangeCAPEX only
$2,400,000 - $3,100,000Lower cash need
$3,845,000Model baseline
$4,600,000 - $5,500,000Highest cash need
Best fit
Best for markets with modest referral volume, mixed payer mix, and a cautious first site.
Best for a site with steady demand, workable payer mix, and a solid physician referral base.
Best for dense referral markets with strong payer mix, high patient demand, and room to scale.
!
Planning note: These scenario ranges are researched planning assumptions, not exact vendor quotes or financing offers.
How much does it cost to open a radiology center?
Opening a Radiology Center is a funding plan, not one universal price: modeled CAPEX is $3.845M, including a $2.95M equipment subtotal before facility and IT. Month 5 cash bottoms at -$2.572M, so pair runway planning with What Is The Most Critical Metric To Measure The Success Of Radiology Center?, not invoice totals alone.
Cost drivers
Fund MRI, CT, X-ray, PACS, EHR, IT
Size spend by scanner count and modality mix
Include buildout, shielding, furnishings, lease terms
Protect cash beyond vendor invoices
Year 1 setup
Hire 1 radiologist
Staff 2 MRI and 2 CT technologists
Add 2 X-ray technologists and 1 nurse
Cover practice manager, front desk, physician liaison
What do MRI and CT scanner costs include for an imaging center?
For a Radiology Center, MRI and CT costs should be split from facility buildout and working capital. A new MRI machine can run about $20M, a CT scanner about $750k, a digital X-ray system about $200k, and a PACS server and software about $150k when it supports the imaging workflow. Year 1 service contracts can equal 35% of revenue, so treat them as operating cost, not initial CAPEX, and expect vendor quotes, room conditions, and service levels to change the final number.
Capital items
New MRI can be about $20M
CT scanner can be about $750k
Digital X-ray can be about $200k
PACS server/software can be about $150k
Cost items to add
Use refurbished vs new pricing carefully
Include installation and calibration
Add coils, workstations, and accessories
Keep service contracts in operating cost
How much funding do I need to open a radiology center?
If you’re opening a Radiology Center, the base case starts around $3.845M CAPEX plus startup cash for payroll, rent, insurance, software, professional fees, reimbursement timing, and payer ramp-up. The model also shows $34,450 in fixed monthly costs, about $954k in Year 1 payroll, and a Month 5 minimum cash of -$2.572M to size the runway. Treat Month 1 operating breakeven, 25-month payback, 0.07% IRR, 641% ROE, and Year 1 EBITDA of $862k as planning outputs, not guarantees.
Cash to open
$3.845M CAPEX to start
Add startup expenses
Fund payroll runway
Cover rent and insurance
Model drivers
Use equipment financing debt
Include depreciation and amortization
Model interest and principal
Keep a cash reserve policy
Key Takeaways
Imaging equipment is the biggest startup cost driver.
Buildout is separate from rent and scanner purchase.
IT launch costs cover PACS, EHR, and cybersecurity.
Year one payroll needs about $954k monthly before benefits.
Radiology Center Core Five Startup Costs
Radiology Equipment Startup Expense
Core gear
The main launch cost is imaging hardware: MRI machine $20M, CT scanner $750k, and digital X-ray system $200k, plus installation, calibration, workstations, coils, accessories, warranties, and setup. The listed items add to $20.95M, so confirm whether the stated $295M subtotal is a typo or includes more equipment.
Price drivers
Build the estimate from units × quoted price, then add install, calibration, and room prep if they are not bundled. Ask if systems are new or refurbished, whether installation is included, what service response time is contracted, and whether modality rooms need special prep. Equipment service contracts are modeled separately at 35% of Year 1 revenue.
Check install is in the quote.
Confirm room prep scope.
Separate service contracts from CAPEX.
Spend control
Use refurbished units only if warranty, calibration, and response times still meet clinical needs. The fastest way to waste money is double-paying for installation, room prep, or service setup that is already in the vendor quote. One clean question saves a lot: what is included, and what is extra?
Compare quoted response times.
Verify bundled accessories.
Avoid duplicate prep work.
Contract check
Before you sign, lock down service response time, who covers breakdowns, and whether the modality room needs special electrical or shielding prep. If those terms are vague, your launch budget can slip fast because repair support, calibration, and site work often show up after the purchase price.
Radiology Facility Buildout Startup Expense
Buildout Scope
Facility buildout is a separate startup cost from scanner purchase price. The researched assumption is $500k over Month 1 to Month 5 for the MRI suite, CT room, X-ray room, shielding, reinforced walls, electrical, HVAC, ADA work, control rooms, changing areas, waiting space, and landlord improvements.
Budget Inputs
Use quotes for room prep, power, and mechanical work, then add $70k for office furniture and fixtures and $40k for patient-area furnishings. Keep these with non-equipment space costs, not scanner CAPEX. One line to remember: the rooms have to work before the scanners can.
Cost Control
Protect the budget by reusing any existing shell work where you can, but do not trim shielding, HVAC, electrical capacity, or ADA items. If the landlord covers some improvements, document it clearly so the $500k buildout line stays clean. That keeps the startup model honest and avoids hiding rent in CAPEX.
Lease Runway
The $20k monthly lease belongs in operating runway, not buildout CAPEX. Over 5 months, that is $100k of cash need before opening, so model it beside pre-opening payroll instead of inside the renovation line.
Radiology Licensing and Accreditation Startup Expense
Launch compliance
Licensing spend covers state radiation registration, facility licensing, payer enrollment, credentialing, written policies, legal formation, radiation safety officer setup, medical physicist testing, and compliance consulting. If you plan accreditation prep for standards some payers use, treat it as a planning line, not a universal mandate. These steps often start before the first scan and can slow opening.
Sizing the spend
Estimate it from permit fees, physicist quotes, legal hours, enrollment count, and the months until approval. Here’s the quick math: $2,000 in monthly professional fees plus $3,000 in insurance equals $5,000 a month in launch-period overhead before claims start paying.
Use state fee schedules.
Quote testing and reviews.
Count approval months.
Trim the bill
Cut waste by bundling consulting, reusing policy templates, and sequencing filings by state priority. Do not pay for full accreditation prep if your payer mix or modality list does not need it yet. Savings usually come from fewer rework hours and fewer rushed filings, not from skipping compliance.
Bundle physicist and legal work.
File high-priority permits first.
Avoid duplicate policy drafts.
Timing risk
What this estimate hides is timing risk: payer enrollment and credentialing can lag, so the center may carry $5,000 a month in fees and insurance before the first claim pays. Local rules, modality mix, and payer contracts decide how fast you need extra prep and whether more review is required.
Radiology Software and IT Startup Expense
Compliance-first IT
Treat imaging IT as compliance-critical workflow infrastructure, not generic office software. The $285k launch subtotal covers PACS (image storage and routing), EHR/EMR integration, workstations, and security. It sits beside, not inside, the $3,500 monthly software run rate starting in Month 1.
Launch subtotal
Budget the subtotal from three inputs: $150k PACS server/software, $75k EHR implementation, and $60k IT infrastructure and workstations, for $285k total. Add RIS, DICOM routing, reporting, billing interfaces, telecom, cybersecurity, backup, and user devices. Ask if billing, referring physician portal, and image exchange are included.
Control scope
Keep scope tight. Price each interface separately and confirm service levels before signing. The usual misses are billing, portal access, and image exchange, which can delay go-live and add rework. The $3,500 monthly subscriptions belong in operating runway, so don’t hide them in launch CAPEX.
Go-live risk
If the system set is complete at launch, the workflow stays smoother and reporting risks drop. If onboarding drags past Month 1, the fixed $3,500 monthly IT burden starts before revenue stabilizes, so lock down integration, backups, and cybersecurity early.
Radiology Staffing and Payroll Startup Expense
Payroll runway
Pre-opening payroll should sit outside steady-state operating payroll. For Year 1, the staff stack totals $1.145M: 1 radiologist at $350k, 2 MRI technologists at $90k each, 2 CT technologists at $85k each, 2 X-ray technologists at $70k each, 1 nurse, 1 manager, 1 front desk coordinator, and 1 physician liaison.
Cost build
Here’s the quick math: add each salary, then divide by 12 for monthly burn. That works out to about $95.4k per month before benefits or payroll taxes if those are not modeled elsewhere. Recruiting, credentialing, onboarding, training, radiologist coverage, billing support, and payer enrollment can all push cash needs up before first scan revenue.
Control burn
Keep the team lean until scan volume is real. Use part-time or shared coverage where allowed, delay nonessential hires, and tie the physician liaison and billing help to referral and claim flow. The big mistake is treating opening month payroll like normal operations. One clean rule: hire for booked volume, not for hoped-for volume.
Pre-open cash
Build a separate runway for the period before cash collections start. Payer enrollment, credentialing, and radiologist coverage can delay billing, so payroll may start before reimbursement does. That makes this cost more than staffing; it’s also timing risk. If opening is delayed, the payroll line keeps running even when scan revenue is still zero.