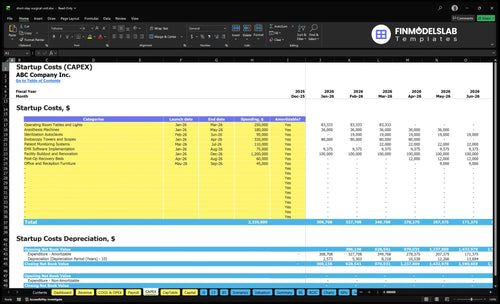
Short-Stay Surgical Center Startup Costs: Plan Around $30M
A short-stay surgical center needs about $30M in planning capital in this model: $2335M of startup CAPEX plus $664k of minimum cash These are researched planning assumptions, not vendor quotes or guaranteed construction bids The biggest CAPEX line is facility buildout and renovation at $1200M, followed by endoscopy towers and scopes at $320k, operating room tables and lights at $250k, and anesthesia machines at $180k Opening-month fixed overhead is $697k before payroll, and Year 1 staffing totals $1180M annually, so the funding plan must cover readiness before reimbursements stabilize
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a short-stay surgical center.
!
What this leaves out This calculator excludes inventory, payroll runway, pre-opening wages, owner pay, working capital, deposits, debt service, financing costs, and other operating expenses. It is for hard startup CAPEX only.
Calculate Fuding Needs
Startup cost summary
This table shows the main startup assets and excluded cash need for a short-stay surgical center.
Highlighted CAPEX$2,045,000Base planning example
Excluded cash needs$664,000Outside CAPEX total
Funding need$2,709,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Facility Buildout and Renovation
$1,200,000
Leasehold buildout, code compliance, and room conversion scope
Yes
Endoscopy Towers and Scopes
$320,000
Scope count, tower spec, and vendor quote spread
Yes
Operating Room Tables and Lights
$250,000
OR table count and lighting package
Yes
Anesthesia Machines
$180,000
Machine count, monitoring package, and installation
Yes
Sterilization Autoclaves
$95,000
Sterilization capacity, service setup, and delivery
Yes
Operating Reserve
$664,000
Month 1 minimum cash, fixed overhead, and Year 1 payroll
Costs move fast when you add rooms, equipment, PACU beds, and staffing depth. Lean fits a phased launch; Base matches the model; Full covers a broader multi-room build.
Lean, Base, and Full funding bands for a short-stay surgical center launch.
Scenario
Lean LaunchPhased start
Base LaunchModel match
Full LaunchExpanded build
Launch model
Starts with one or two rooms, defers some equipment, and keeps staffing lean while proving procedure mix.
Uses the researched model with the planned room mix, core equipment, and opening staffing built for steady same-day volume.
Starts multi-specialty, multi-room, with deeper recovery capacity and more equipment from day one.
Typical setup
Uses a smaller buildout, thinner opening inventory, and limited PACU capacity.
Covers the modeled CAPEX, opening cash, and the staffing depth needed for the Year 1 plan.
Adds more rooms, PACU beds, broader inventory, and heavier accreditation and support costs.
Cost drivers
Fewer rooms
deferred equipment
thinner inventory
lighter staffing
smaller buildout
Core buildout
full equipment set
opening cash
modeled staffing
accreditation work
More rooms
PACU capacity
extra equipment
deeper inventory
broader accreditation
Planning rangeCAPEX only
$1.6M - $2.2MLower capital
$2.3M - $3.0MBase case
$3.1M - $4.2MHigher capital
Best fit
Best for founders testing one specialty or a narrow procedure list before scaling.
Best for operators funding the full base case and aiming to open at the planned scale.
Best for teams with enough capital to launch broader procedure mix and absorb a slower ramp.
!
Planning note: These ranges are researched planning assumptions, not exact vendor quotes or bids.
What drives the cost of opening an ambulatory surgery center?
Opening a Short-Stay Surgical Center is driven mostly by regulated clinical buildout, not rent. The model’s biggest line is the $1,200M buildout, then $320k for endoscopy towers and scopes, $250k for OR tables and lights, $180k for anesthesia machines, $110k for monitors, and $95k for autoclaves. That’s because the site needs code-compliant rooms, sterile processing, PACU bays, medical gas, HVAC, life safety, information systems, and accreditation readiness.
Main cost drivers
Number of ORs sets buildout size
Procedure mix drives equipment needs
Specialty gear adds large capex
PACU bays need extra space
Systems you must fund
Sterile processing needs autoclaves
Medical gas and HVAC are required
Life safety and IT add cost
Accreditation readiness is not optional
How much capital is needed to open a short-stay surgical center?
A Short-Stay Surgical Center needs about $3.0M in startup funding before opening: $2.335M for CAPEX plus $664k minimum cash. That cash matters because payroll, fixed costs, contracting, and reimbursement lag hit before collections stabilize; see What Are The 5 KPIs For Short-Stay Surgical Center? for the operating metrics that protect that runway.
Startup Uses
$1.200M facility buildout
$320k endoscopy systems
$250k OR tables and lights
$180k anesthesia machines
Cash Need
$75k EHR implementation
$664k minimum working cash
$10.865M Year 1 revenue assumption
22.1% of funding held as cash
How should founders fund an ambulatory surgery center startup?
For a Short-Stay Surgical Center, fund the build with a clear sources-and-uses plan, a CAPEX schedule, and enough cash to cover launch timing, payer reimbursement lag, and the staffing ramp. The base case points to about $30M in minimum cash before any financing buffer, and the pro forma shows Month 1 breakeven plus a one-month payback under researched assumptions.
Fund the build
Plan CAPEX by month.
Match debt to launch timing.
Hold cash for reimbursement lag.
Add buffer above $30M.
What lenders check
Test procedure volume.
Review physician pipeline.
Stress-test payer mix.
Validate $10.865M revenue and $7.220M EBITDA.
Key Takeaways
Buildout and renovation are the biggest upfront CAPEX driver.
Equipment is reusable CAPEX, not disposable supply cost.
Year one staffing runs about $1.18M annually.
Supplies and accreditation costs scale with procedure mix.
Short-Stay Surgical Center Core Five Startup Costs
Facility Buildout and Renovation Startup Expense
Buildout Budget
Facility buildout is a hard-cost CAPEX line, and this plan sets it at $1,200M from Month 1 through Month 12. The real driver is site condition: a leased shell costs less to convert than a medical space, but both still need the right clinical layout, operating rooms, and code-ready systems.
What It Covers
This spend covers operating rooms, procedure rooms, sterile corridors, pre-op and recovery flow, HVAC, medical gas, life safety, accessibility, plumbing, electrical load, backup systems, and state or local code fixes. To size it, use square footage, number of ORs, procedure mix, certificate or licensure pathway, landlord allowances, and inspection milestones.
Leased shell or medical conversion?
How many ORs and procedure rooms?
Which code and licensing path?
How To Control It
Lock the scope early, because late layout changes can trigger pricey change orders. The best way to protect this budget is to match the room plan to the procedure mix, get landlord allowances in writing, and tie spending to permit and inspection steps. That keeps the build from drifting past what the center truly needs.
Freeze room count before permit
Price allowances in the lease
Track every inspection date
Build Timing Risk
Buildout cash does not move in a straight line. Site review, rough-in, final inspection, and the certificate or licensure pathway can push spend across the full 12-month window, so the budget only works if contractor draws and approval milestones stay synced.
Medical Supplies and Opening Inventory Startup Expense
Opening Inventory
For an ASC, opening inventory is a real cash sink: the source model sets medical and surgical supplies at 120% of Year 1 revenue and sterilization and laundry at 30%. With Year 1 revenue at $10,865M, supply demand is very sensitive to case mix, even if opening stock is not quoted separately.
What It Covers
This line covers instrument sets, trays, disposables, sterile packs, drugs, emergency supplies, and implants when used. Estimate it from units × unit price, then add vendor stocking and par levels for the first weeks of cases. The key inputs are monthly case count, specialty mix, and how many procedure days you want on hand.
How To Control It
Keep inventory tight by setting par levels by specialty and using vendor stocking for fast movers. Orthopedics at $4,500 per case needs more trays, implant coordination, and backup stock than gastroenterology at $1,200 or pain management at $900. The savings come from fewer slow items, not from cutting critical sterile supply.
Mix Drives Spend
Procedure mix drives the bill more than the word inventory. A center weighted to orthopedics will carry pricier, less reusable items, while GI and pain cases usually need lighter kits and fewer implants. If opening stock is planned from case mix, the first question is which specialties fill the schedule in Month 1.
Operating Room and Clinical Equipment Startup Expense
Equipment CAPEX
Operating room and clinical equipment is reusable startup CAPEX, not supply spend. For a basic ambulatory surgery center, the listed lines total about $1.015M: tables and lights $250k, anesthesia machines $180k, endoscopy towers and scopes $320k, monitoring systems $110k, autoclaves $95k, and recovery beds $60k.
Cost Drivers
Price swings come from specialty mix, room count, and whether you buy new or refurbished gear. More ORs, more anesthesia needs, and more recovery bays raise the bill fast. Here’s the quick math: ask vendors for unit quotes by room and by specialty, then add service contract costs and emergency backup items before you lock the budget.
Quote by room, not by guess
Split new vs refurbished
Price service separately
Save Without Risk
Cut cost by using refurbished equipment where service history is solid and the device is not safety-critical. Don’t bury implants, sterile packs, drugs, or disposable procedure supplies in this line. The smart move is to protect uptime on anesthesia, monitoring, and sterilization gear, because one failed device can cost more than the savings.
Budget Guardrail
Build the equipment plan around the actual procedure mix. Endoscopy-heavy centers need more tower and scope spend, while higher-acuity cases push anesthesia, monitoring, and emergency equipment higher. The right model is units × vendor quote × room count, plus service and installation. That keeps equipment CAPEX clean and stops supply costs from inflating the build.
Staffing Readiness and Pre-Opening Payroll Startup Expense
Staffing Budget
Treat staffing readiness as pre-opening payroll and working capital, not CAPEX. Year 1 payroll totals $1.18M, or about $98.3k per month, for 1 administrator, 1 director of nursing, 6 registered nurses, 4 surgical technologists, 2 medical coders and billers, and 2 receptionists. This spend gets the center ready before revenue starts.
Cost Build
Estimate this with headcount × annual pay, then add months of pre-opening coverage. The listed salaries are $145k, $125k, 6 × $85k, 4 × $55k, 2 × $50k, and 2 × $40k. It also covers recruiting, credentialing, onboarding, training, policy drills, physician scheduling, and anesthesia coordination.
Cost Control
Keep the team lean until licensure and room readiness are locked. Stagger start dates, use temporary help for admin work, and hire RNs and front-desk staff close to opening. Don’t cut credentialing or drills; one failed schedule, payer setup, or anesthesia handoff can cost more than a few weeks of payroll.
Readiness Timing
The real risk is paying staff too early. If opening slips, working capital burns fast, so tie hiring to inspection milestones and surgeon block schedules. One clean rule: hire for the next 30 to 60 days of readiness, not the next year of optimism.
Licensing, Accreditation, and Professional Services Startup Expense
Monthly Run Rate
For a short-stay surgical center, this line item runs at $25k a month for licensing and accreditation plus $12k for professional liability insurance, or $37k monthly. That is $444k a year before the first case. It covers state licensure and Centers for Medicare & Medicaid Services certification prep, not just filing fees.
What It Covers
This budget pays for legal entity setup, architectural review, clinical policies, compliance consulting, credentialing documentation, inspection prep, and payer strategy. One line: paperwork, review, and readiness. The exact spend depends on state licensure rules, ownership structure, specialty mix, and whether the center seeks Medicare and commercial payer contracts.
State licensure path
CMS certification prep
Accreditation readiness
Budget Inputs
Estimate it as months of coverage × $37k, then add any outside quotes for legal, compliance, and insurance work. The key inputs are the approval timeline, number of review cycles, and whether the center needs payer contracts. More specialties and more payers usually mean more documentation and more inspection prep.
Months to approval
Consultant quote scope
Payer contract target list
Control the Burn
Use a fixed-fee scope for compliance consulting, credentialing, and inspection prep, and keep the licensure path as narrow as your business model allows. Don’t skimp on policies or readiness testing; rework is expensive. The cleanest savings come from avoiding delay, because every extra month adds $37k before operations start.