Telemedicine Startup Costs: Plan On $280K CAPEX Plus Cash Runway
Telemedicine
You’re budgeting a phone or video consultation service, so separate core startup costs from cash runway This outline covers $280,000 in CAPEX, compliance setup, technology, licensing, insurance, staffing readiness, marketing launch, and working capital, with $661,000 minimum cash in Month 12 and break-even in Month 13 Ongoing operating losses, owner salary, debt service, and growth funding are separate from core startup costs
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimate capitalized startup assets for a telemedicine launch, including build, setup, and equipment costs only.
!
CAPEX only This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, deposits, debt service, working capital, monthly SaaS fees, insurance premiums, marketing spend, and other operating costs.
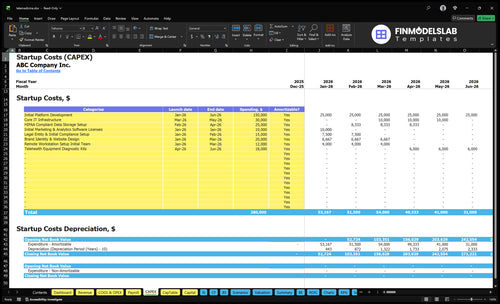
What should the Telemedicine CAPEX screenshot show?
For Telemedicine, initial platform development drives cost the most at $150,000, especially when you build secure video, patient intake, scheduling, payment flow, admin dashboards, audit controls, cybersecurity, data storage, and EHR connection. After that, core IT infrastructure is $30,000 and HIPAA-compliant data storage setup is $25,000; monthly tech spend then adds $5,000 for maintenance and hosting, $1,200 for compliance software, and $1,500 for cybersecurity services. In Year 1, scalable technology costs run at 0.8% of revenue, so higher visit volume still pushes spend up.
Big build costs
$150,000 platform development
Secure video takes the most depth
Patient intake and scheduling add work
EHR connections raise scope fast
Recurring tech spend
$5,000 monthly maintenance and hosting
$1,200 monthly compliance software
$1,500 monthly cybersecurity services
0.8% of Year 1 revenue
How much does it cost to launch a telemedicine company?
Launching Telemedicine costs about $280,000 in core CAPEX (upfront build spend) and up to $661,000 in total cash need by Month 12. The key choice is lean single-state launch versus broader multi-provider or multi-state setup; tie that choice to What Is The Most Important Indicator Of Success For Telemedicine?. In the base case, Year 1 starts with 13 practitioners, posts -$20,000 EBITDA, and breaks even in Month 13.
Startup costs
$150,000 platform development
$25,000 HIPAA-compliant storage
$15,000 compliance setup
$20,000 website and brand
Post-launch burn
$18,000 diagnostic kits
$10,850 monthly fixed overhead
$457,500 Year 1 payroll
13 providers across 5 categories
How should telemedicine startup funding connect to the financial model?
For Telemedicine, funding should follow the model: start with $280,000 in CAPEX, add $10,850 a month in fixed overhead, and cover $457,500 in Year 1 staffing. The model also shows 753 monthly consultations at capacity, about $64,725 in monthly revenue before ramp timing, break-even in Month 13, and payback in 18 months. Year 1 EBITDA is about -$20,000, so the funding ask is a runway plan, not a product pitch.
Funding need
$280,000 CAPEX upfront
$10,850 monthly fixed overhead
$457,500 Year 1 staffing
Model runway before revenue ramps
Model checks
753 monthly consultations at capacity
About $64,725 monthly revenue
58% variable costs and 120% COGS in Year 1
Month 13 break-even, 18-month payback
Calculate Fuding Needs
Startup cost summary
This table shows startup CAPEX ranges for telemedicine plus excluded cash runway needed before breakeven.
Highlighted CAPEX$243,000Base planning example
Excluded cash needs$661,000Outside CAPEX total
Funding need$904,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Initial Platform Development
$150,000
Build of the remote consultation platform
Yes
Core IT Infrastructure
$30,000
Servers, hosting, and core systems
Yes
HIPAA-Compliant Data Storage Setup
$25,000
Secure storage and compliance setup
Yes
Brand Identity and Website Design
$20,000
Launch branding and web build
Yes
Telehealth Equipment and Diagnostic Kits
$18,000
Remote exam tools and starter kits
Yes
Operating Reserve
$661,000
Month 12 cash runway before breakeven
No
Telemedicine Core Five Startup Costs
Technology Platform and Implementation Startup Expense
Build Budget
The telemedicine platform is the largest upfront spend. The source plan totals $215,000 in one-time setup from Month 1 to Month 6: $150,000 platform development, $30,000 core IT infrastructure, $25,000 HIPAA-compliant (Health Insurance Portability and Accountability Act) storage, and $10,000 software licenses for launch tools.
Cost Drivers
Price the workflow, not just the screen. The estimate should separate custom build, integration, multilingual intake, prescription workflow, and payer billing. One line says it all: more clinical steps means more months, more testing, and a bigger quote. Ask vendors for scope, users, and data volume before you commit.
Split build from integration.
Quote multilingual intake separately.
Price billing rules by workflow.
Monthly Run-Rate
Keep setup and recurring costs apart. The fixed monthly base is $5,000 for platform maintenance plus $1,200 for HIPAA compliance software, before hosting and any 8% Year 1 scalable technology cost. That means at least $6,200 per month, so cash planning has to cover both launch and steady state.
Track maintenance as fixed overhead.
Renew compliance tools monthly.
Model scale spend separately.
Scope Check
If the model needs a custom build plus EHR connection, budget toward the high end and get firm quotes before Month 1 starts. Ask vendors to price video, intake, scheduling, payments, admin dashboards, reporting, and storage as separate line items so you can see what is fixed, usage-based, and deferrable.
Regulatory, Legal, Licensing, and Credentialing Startup Expense
Launch Legal Setup
Plan on $15,000 for entity formation and initial compliance setup in Months 1-2, plus $1,000 a month from Month 1 through Month 60. This bucket covers state licensing, HIPAA documents, informed consent, payer enrollment, and provider credentialing, but it still needs attorney and compliance confirmation.
Cost Drivers
Here’s the quick math: the bill grows with the number of states, provider specialties, payer contracts, controlled substance policies, minors’ care, and prescription workflows. Cash-pay models need less payer work than insurer billing. More states and more billable clinicians mean more legal review, credentialing files, and document updates.
More states, more filings
More payers, more enrollment
More specialties, more review
Keep It Tight
Start with the fewest states and the fewest clinical lines that still work. Use attorney-drafted templates for informed consent, HIPAA, and clinical documentation rules, then adapt them only where required. The biggest waste is paying to rewrite the same compliance pack for every new state or payer.
Monthly Compliance
The model’s ongoing legal and regulatory line is $1,000 per month. Treat it as core overhead, not a one-time fee, because licensing, credentialing, and documentation rules can keep changing as you add states, clinicians, or insurer billing.
Insurance and Risk Management Startup Expense
Core cover
For telemedicine, buy professional liability (malpractice), general liability, cyber liability, and workers’ compensation; add D&O if you raise outside capital. The model includes $800/month for general liability and malpractice plus $1,500/month for cybersecurity services. Any upfront premium or deposit should sit in working capital, not just monthly expense.
Price drivers
Premiums change with specialty, state, claims history, provider employment model, and visit volume. Psychiatry, dermatology, pediatrics, and primary care can price differently, so get quotes by service mix, not one blended rate. If you use W-2 clinicians, workers’ comp matters more; if you use contractors, confirm how liability is split.
Quote each specialty separately
Check state-by-state rules
Match coverage to clinician model
Cyber needs
Cyber coverage should map to protected health information, payment workflows, secure storage, and breach response planning. The $1,500 monthly cyber spend is more than software; it supports access controls, logging, backups, and incident response. If you store records or process payments, underwriters will want proof of those controls.
Document PHI handling
Show payment data flow
Keep breach steps ready
Capital item
If you’re raising outside capital, add D&O so board and officer claims don’t hit founders personally. Ask whether the quote needs an upfront deposit, annual prepay, or monthly billing, because that changes cash on hand. Don’t buy a cheap policy that excludes the exact telehealth services you sell.
Staffing Readiness and Clinical Operations Startup Expense
Launch Team
Launch staffing starts with 5 general physicians, 3 pediatricians, 2 dermatologists, 2 psychiatrists, and 1 nutritionist. Internal payroll is $457,500 for the CEO, CTO, Head of Operations, customer support lead, and marketing manager. Keep these fixed salaries separate from practitioner payouts, which are modeled at 110% of revenue in Year 1.
Onboarding Costs
This bucket covers recruiting, background checks, credential files, training, clinical protocols, medical director time, support scripts, and patient escalation rules. The clean way to budget it is to list each role, each check, and each onboarding step, then split one-time setup from ongoing staffing. That keeps launch payroll deposits from hiding true startup burn.
Cost Control
Batch onboarding by specialty, reuse scripts, and require credential files before scheduling. That cuts rework without weakening compliance. Do not mix hiring readiness with revenue-based practitioner pay; the first is a launch cost, the second scales with visits. If volume ramps fast, this line item still needs room for support coverage.
Payroll Mix
The fixed base is $457,500, but Year 1 economics still swing on volume because practitioner payouts sit at 110% of revenue. That means every new visit must cover support load and clinician cost, not just software. The startup budget should flag this as a staffing-readiness item, not a simple payroll line.
Patient Acquisition and Launch Marketing Startup Expense
Launch Spend
In a direct-to-consumer telemedicine model, patient acquisition is not optional. Plan a $30,000 launch base: $20,000 for brand identity and website design in Months 1-3, plus $10,000 for marketing and analytics software in Month 1. That funds the site, landing pages, search engine optimization (SEO), paid search tests, referrals, and launch campaigns.
Test Budget
Use revenue to set the monthly test budget. Year 1 marketing and patient acquisition equals 50% of revenue, then 45% in Year 2 and 40% in Year 3. One line: if you do not fund demand, booked visits stall. Track spend by channel and move budget only where visits actually book.
Track booked visits by channel
Review monthly spend against revenue
Cut weak tests fast
Visit Cost
Cost per booked visit is total marketing spend divided by booked visits. Once actual data exists, use that number to judge paid search, referral outreach, and launch campaigns. If bookings are thin, fix targeting and landing pages first. What this estimate hides: no-shows, refunds, and channel lag.
Track Volume
Expected consultation volume should be the count of booked visits once live data starts flowing, not a guess. Build the first forecast from launch spend, monthly test spend, and channel conversion data, then reset it after the first 30 days so every dollar ties back to visits, not clicks.
Compare 3 Startup Cost Scenarios
Scenario table
Lean, base, and full launches change telemedicine startup cost fast because state count, provider depth, compliance load, and marketing spend all scale together.
Lean, base, and full telemedicine launch cost comparison.
Scenario
Lean LaunchBest for cash-pay pilot
Base LaunchBest for multi-specialty launch
Full LaunchBest for funded growth
Launch model
Start with one state, fewer clinicians, and a simple phone or video flow so cash burn stays low while you test demand.
Use the source model as the standard launch plan with enough staff, systems, and marketing to support Year 1 scale.
Build for multi-state coverage and more service lines from day one, with higher spend on systems and provider rollout.
Typical setup
A single-state cash-pay pilot with a small provider panel, basic insurance, and limited integrations.
The model launch uses 13 Year 1 practitioners, $280,000 CAPEX, $10,850 monthly fixed overhead, $457,500 Year 1 internal payroll, and Month 13 break-even.
A broader rollout adds states, more specialties, EHR connections, payer credentialing, stronger cyber controls, and heavier provider onboarding.
Cost drivers
single-state scope
few providers
basic insurance
light marketing test
limited integrations
13 Year 1 practitioners
$280,000 CAPEX
$10,850 monthly fixed overhead
$457,500 Year 1 payroll
Month 13 break-even
multi-state licensing
more specialties
EHR connections
payer credentialing
direct-to-consumer marketing
Planning rangeCAPEX only
Below base CAPEXLower cash need
$280,000 CAPEXBase case
Above base CAPEXHigh build
Best fit
Best for founders testing demand before they add more states, specialties, and compliance layers.
Best for teams that want a balanced launch with clear cash needs and a known break-even path.
Best for funded teams that need broader coverage, payer workflows, and faster scale.
!
Planning note: Scenario ranges are researched planning assumptions, not exact vendor quotes or fixed offers.
Reserve enough to cover the gap between launch spending and break-even In this model, minimum cash reaches $661,000 in Month 12, while break-even comes in Month 13 That cash need sits on top of the $280,000 CAPEX budget and covers the early ramp-up period, fixed overhead, payroll timing, and slower-than-planned patient volume
Not for the core virtual care model in this plan, but you still need operating infrastructure The budget includes $12,000 for remote workstation setup, $750 per month for virtual office and admin tools, and $30,000 for core IT infrastructure If you add a clinic, exam space, or in-person diagnostics, that becomes a separate facilities budget
State licensing is a planning item you should confirm with healthcare counsel before launch The model includes $15,000 for legal entity and initial compliance setup plus $1,000 per month for legal and regulatory compliance fees Costs can rise when you add states, payer enrollment, pediatric care, psychiatry, prescribing workflows, or more credentialed providers
This model reaches break-even in Month 13 and payback in 18 months Year 1 EBITDA is -$20,000, then improves to $1053 million in Year 2 The swing depends on patient volume, practitioner coverage, pricing from $75 to $150 per consultation, and keeping fixed monthly overhead near the planned $10,850 level
Start narrower before adding states, specialties, and deep integrations The biggest CAPEX line is $150,000 for platform development, followed by $30,000 for IT infrastructure and $25,000 for HIPAA-compliant data storage A focused launch can also reduce credentialing work, provider onboarding, insurance scope, and paid marketing tests while you validate patient demand
About the author
Anthony Ross
Independent Business Researcher
Anthony Ross is an independent business researcher at Financial Models Lab who writes practical guides for first-time entrepreneurs planning their first business. Focused on small business money management, he helps readers organize broad business ideas into clear planning assumptions, with straightforward revenue and profit examples that make financial thinking easier to apply.
Choosing a selection results in a full page refresh.