 Owner income$1.1M-$19.7M
Owner income$1.1M-$19.7MHow Much Rehab Center Owners Make: $392M Year 1 Revenue Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$1.1M-$19.7M  Net margin54%-80%
Net margin54%-80% Revenue for target pay$135M
Revenue for target pay$135M Business difficultyHard
Business difficultyHard


Key Takeaways
- Higher census spreads $378k monthly overhead faster.
- Payer mix and rates drive cash and collections timing.
- Staffing is the biggest controllable margin pressure.
- Admissions cost matters, but must stay compliant.
Owner income$1.1M-$19.7MNet margin54%-80%Revenue for target pay$135MBusiness difficultyHardWant to test your rehab center owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay for a rehab center.
Planning note: This is a researched planning estimate only. Actual owner income is not guaranteed and depends on revenue, margins, payroll, taxes, debt, reserves, and distributions. It is not tax advice or owner distribution advice.
How do you check owner income in the Drug and Alcohol Rehab Center model?
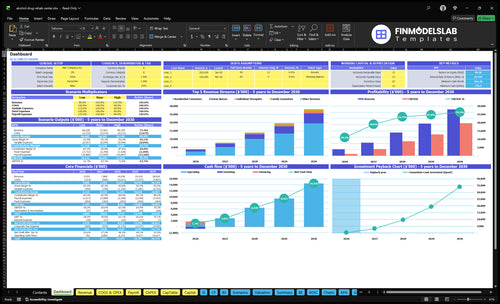
Open the Drug and Alcohol Rehab Center Financial Model Template to see the dashboard, assumptions, and owner income outputs fast.
Owner-income model highlights
- Dashboard and income outputs
- Break-even and cash flow
- Assumptions, staffing, payer mix
What costs most affect rehab center profit margin?
For a Drug and Alcohol Rehab Center, the biggest margin hits are payroll, fixed facility overhead, and revenue-based costs like marketing, supplies, and specialist consults. In Year 1, payroll is $655k, fixed overhead is $4.536M, and variable costs run at 18% of revenue; for startup costs, see What Is The Estimated Cost To Open A Drug And Alcohol Rehab Center?
Biggest cost drivers
- Payroll: $655k in Year 1
- Fixed overhead: $4.536M
- Variable costs: 18% of revenue
- Marketing: 8% falling to 6%
Other margin pressures
- Medical supplies and pharma: 5% to 4%
- Food: tracks with client volume
- Specialist consultations: use only as needed
- Staffing and compliance: planning inputs only
How do owner role, facility type, and scale change income?
For a Drug and Alcohol Rehab Center, owner-operated models can keep management costs down, but they raise execution risk if the owner is stretched thin. Management-run models need more overhead before any distributions, and scale only helps if controls and cash reserves keep up. Residential programs can assume $15,000 per treatment in Year 1, but they also carry facility, food, staffing, insurance, and reserve costs; outpatient therapy is lower at $150 to $250 per visit and is easier to scale with less facility intensity.
Owner role
- Owner-operated cuts management pay.
- Execution risk rises fast.
- Management-run adds overhead first.
- Distributions come later.
Facility and scale
- Residential can price high.
- Year 1 can hit $15,000 per treatment.
- Outpatient runs at $150 to $250.
- Multi-site needs controls and reserves.
What can a rehab center owner take home?
A Drug and Alcohol Rehab Center owner can’t treat operating profit as take-home: Year 1 shows $392M revenue and $211M operating profit before owner pay, taxes, debt, reserves, reinvestment, and unlisted staff roles. Use What Is The Current Growth Trajectory Of Your Drug And Alcohol Rehab Center? to test whether census and payer mix support safe owner draws.
Before Owner Pay
- $655k listed payroll
- $4,536k fixed overhead
- 18% variable costs
- Taxes, debt, reserves still unpaid
What Moves Take-Home
- Keep census steady
- Watch payer mix
- Control staffing gaps
- Reserve cash despite $2,802M mature revenue
Want the six rehab center income drivers?
1
25%-85%Occupancy
When census climbs from 25% to 85%, the same rooms and core staff earn far more treatment days, so owner take-home rises first.
2
$150-$17KPayer Mix
Higher reimbursement on the same care mix drops more revenue to the bottom line because staffing does not rise one for one.
3
8-90/moProgram Mix
Shifting mix toward higher-value programs lifts revenue per clinician hour, while low-volume services need tight scheduling to avoid drag.
4
1-12 FTEStaffing Load
Keeping FTEs close to census protects margin, because idle labor and overtime cut owner take-home fast.
5
8%-6%Acquisition Cost
Driving marketing and acquisition from 8% to 6% keeps more of each admission dollar in the business during ramp.
6
$779KCash Buffer
The Month 6 cash trough of about $779K is the reserve line, and thin cash can block owner draws even when EBITDA is rising.
Drug and Alcohol Rehab Center Core Six Income Drivers
Occupancy and census
Occupancy and Census
Occupancy is what turns licensed capacity into revenue. In Year 1, modeled census runs at 25% to 40% by service, so fixed overhead like rent, insurance, utilities, and security still sits on a thin revenue base. By Year 5, census rises to 70% to 85%, so each filled slot spreads the $378k per month overhead across more billable care and lifts owner income faster.
Here’s the quick math: if census moves up while pricing and staffing stay controlled, contribution margin improves fast after break-even. The risk is simple, though: never model volume above licensed or operational limits. Inputs needed are licensed capacity, average daily census, service-specific occupancy, admissions, and discharges. More filled capacity usually means better cash flow and more room for owner draw, but only when care is staffed well.
Track Census by Service Line
Measure daily census against licensed capacity, not just total admissions. Watch occupancy by detox, residential, and therapy services, because a higher census in one line can hide empty beds in another. If census is below 25% to 40% in Year 1, fixed costs eat margin fast; if it reaches 70% to 85%, each added client helps cover the $378k monthly overhead.
- Track daily filled beds or slots.
- Compare census to licensed capacity.
- Watch admissions, discharges, and no-shows.
- Cap volume at operational limits.
- Test how one extra client changes profit.
1
Payer mix and reimbursement
Payer Mix and Net Collections
Payer mix is the share of clients paid by commercial insurance, private pay, Medicaid, and denied claims. It drives net collections and cash timing, so the same billed services can produce very different owner income. In Year 1, the model uses charge assumptions of $5,000 detox, $15,000 residential, $150 individual therapy, $250 family counseling, and $300 medical doctor services.
For modeling, treat payer mix, negotiated rates, denial rate, and collection lag as separate inputs. That matters because reimbursement is not the same as billed price. If cash comes in slowly, operating profit can look fine while owner draws stay tight. One clean rule: revenue is booked fast, cash is not.
Track Realized Rate and Days to Cash
Build the forecast from service volume × charge × expected collection rate, then layer in timing. Track realized rate by payer and by service line, plus denials, write-offs, and days in accounts receivable. That shows which payers support margin and which ones delay owner pay.
- Split commercial, private pay, Medicaid.
- Track denial rate monthly.
- Measure cash lag by payer.
- Reforecast after contract changes.
This is financial modeling, not reimbursement advice. Still, the owner should test how much cash remains after slow payers, because collections timing can force more working capital even when census and charges are strong.
2
Program and service mix
Service Mix
The mix is the share of detox, residential, and outpatient-style sessions you sell. It changes revenue per client and the cost load behind it. In the model, residential runs $15,000 per treatment in Year 1 and $17,000 in Year 5, detox is $5,000 to $5,500, and outpatient sessions are $150 to $330 in Year 1.
One residential case brings about 3x the revenue of a $5,000 detox case, but it can also bring more medical, food, facility, and staffing cost. So owner pay depends on contribution margin, not just ticket size. A richer mix can lift profit, but only if the added care level stays within staffing and room capacity.
Track Margin by Program
Build a simple report by service line: clients, price, direct staff hours, meds, food, and room cost. Here’s the quick test: compare revenue per treatment against variable cost per treatment, then see what is left to cover fixed overhead and profit draw. Do not choose programs only for margin; clinical fit still comes first.
- Price each service separately.
- Track direct cost per treatment.
- Watch cash by program.
3
Clinical staffing model
Clinical Staffing Load
Staffing is the biggest controllable margin pressure after census. Listed payroll starts at $655k in Year 1 from the clinical director, detox nurses, and residential counselors, then climbs to $132M by Year 5 as headcount grows from 3 to 6 detox nurses and 5 to 12 residential counselors. If labor rises faster than paid volume, gross margin and owner take-home drop fast.
The model also needs credentialed clinicians, nursing, case management, admissions, and management to match capacity. Here’s the key risk: staffing too early hurts cash flow, but staffing too late hurts care quality and revenue. No staffing compliance rules were provided, so the cleanest control is labor aligned to licensed capacity and actual census.
Match Labor to Capacity
Track labor per occupied bed day, overtime, and any agency use by role. Build the schedule from census, not hope. One unfilled shift or one extra hire can move monthly profit more than a small pricing change, because payroll is fixed before collections hit the bank.
- Census by service line
- Paid hours by credential
- Overtime and agency coverage
- Admissions lag by week
Use the staffing plan to test break-even by scenario: if census dips, pause nonessential hiring; if census holds, add coverage where client hours are tightest. The owner’s income improves when the team stays right-sized and every staffed hour supports billable care.
4
Admissions and acquisition cost
Admissions and acquisition cost
Admissions turn inquiry volume into census, but the spend can cut margin fast. The model sets marketing and client acquisition at 8% of revenue in Year 1 and 6% by Year 5, with the provided dollar figures at $3,135k on $392M revenue and $168M on $2,802M revenue. The owner only wins if each admit covers its own acquisition cost.
Track lead cost, call conversion, referral quality, admissions staffing, and trust. If lead flow is weak or admissions are slow, cash gets tied up before collections land, and profit drops even when census looks healthy. Keep acquisition planning compliant and avoid improper referral incentives.
Track the intake math
Here’s the quick math: measure cost per lead, cost per admit, and admit-to-start conversion by source. If one referral channel brings better-fit clients, it can lower total acquisition cost even with a higher lead price. What this estimate hides is denied claims, no-shows, and long sales cycles.
- Review source conversion weekly.
- Measure staffed calls per day.
- Document all referral payments.
- Remove tied-to-volume incentives.
Use a fast callback process, a clear intake script, and tight handoffs from admissions to clinical staff. In this business, a small lift in conversion can matter more than chasing cheap leads, because better trust usually means steadier census and more reliable owner pay.
5
Fixed overhead, reserves, and financing
Fixed overhead and owner cash
$378k in monthly fixed overhead is the cash drag here: $25k lease, $45k utilities, $3k insurance, $2k maintenance, $1k licensing and accreditation, $800 software, and $15k security. That totals $4,536k a year. Operating profit is not owner cash, because debt service, taxes, reserves, maintenance, working capital, and reinvestment come first.
The key input is monthly net cash after fixed costs, not just revenue. If census or collections slip, the fixed base still lands every month, so owner pay can drop to zero even when profit looks fine. One clean rule: if the business cannot cover fixed overhead plus reserves, distributions should wait.
Track cash before distributions
Build a monthly cash bridge that starts with collections, then subtracts payroll, fixed overhead, debt service, taxes, reserves, and reinvestment. Track reserve balance and the point where cash in covers cash out. That tells you what is really available for owner pay while the center stays open and compliant.
- Track overhead monthly.
- Stress test lower census.
- Set reserves before draws.
6
Scenario objective: compare low, base, and high rehab center owner income assumptions
Owner income scenarios
Capacity and staffing drive owner income here. The lean year 1 ramp, base year 3, and high year 5 show how margin improves as occupancy fills.
| Scenario | Lean CaseLean | Base CaseBase | High CaseHigh |
|---|---|---|---|
| Launch model | Year 1 ramp keeps owner income lower while capacity moves from 25% to 40%. | Year 3 creates a steadier owner income path with mid-range capacity and margin. | Year 5 supports the strongest owner income path as capacity and margin peak. |
| Typical setup | Revenue is modeled at $392M with 18% variable costs, $655k listed payroll, and $4.536M fixed overhead before owner pay. | Revenue is modeled at $1,404M with 16% variable costs and $1,035M operating profit before owner pay. | Revenue is modeled at $2,802M with 14% variable costs and $2,232M operating profit before owner pay. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $211MLean case | $1.035BBase case | $2.232BHigh case |
| Best fit | Use this to stress-test a slower start and heavier cost load. | Use this as the main planning case for a stabilized operation. | Use this to test upside if utilization stays high and costs stay tight. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. They exclude taxes, debt, reserves, unlisted payroll, and guarantees.
Related Products
- Drug and Alcohol Rehab Center Porter's Five Forces Analysis
- Drug and Alcohol Rehab Center BCG Matrix
- Drug and Alcohol Rehab Center Business Model Canvas
- 7 Critical KPIs for Drug and Alcohol Rehab Centers
- Drug And Alcohol Rehab Center Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Drug and Alcohol Rehab Center Profitability
- How Much Does It Cost To Run A Drug and Alcohol Rehab Center Monthly?
- How Much It Costs To Open A Drug And Alcohol Rehab Center: $779K Plan
- Drug and Alcohol Rehab Center Financial Model Template in Excel
- How to Open a Drug and Alcohol Rehab Center in 6 to 12+ Months
- How to Write a Drug and Alcohol Rehab Center Business Plan
- Drug and Alcohol Rehab Center Marketing Mix
- Drug and Alcohol Rehab Center Marketing Plan
- Drug and Alcohol Rehab Center Business Proposal
- Drug and Alcohol Rehab Center PESTEL Analysis
- Drug And Alcohol Rehab Center Pitch Deck Example Editable PPTX
- Drug and Alcohol Rehab Center Business SWOT Analysis
- Drug and Alcohol Rehab Center Value Proposition Canvas
Frequently Asked Questions
Owner income depends on census, payer mix, staffing, and reserves In the provided first-year model, revenue is $392M, variable costs are 18%, listed payroll is $655k, and fixed costs are $4536k The remaining $211M is operating profit before owner pay, taxes, debt, reserves, reinvestment, and unlisted staffing costs