 Owner income$3.3M
Owner income$3.3MHow Much Does an ASC Owner Make? $35M First-Year Cash Flow

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$3.3M  Net margin53%
Net margin53% Revenue for target pay$6.3M
Revenue for target pay$6.3M Business difficultyHard
Business difficultyHard


An ASC owner’s take-home is usually estimated from facility profit, then reduced for debt service, taxes, reserves, and the owner’s equity share In this model, first-year revenue is $647 million and EBITDA is $350 million, a 541% margin before owner-level items By the mature year, modeled revenue reaches $3974 million with $3079 million of EBITDA These are planning assumptions, not salary guarantees
Owner income$3.3MNet margin53%Revenue for target pay$6.3MBusiness difficultyHardWant to estimate your ASC owner take-home?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Ambulatory Surgery Center financial model?
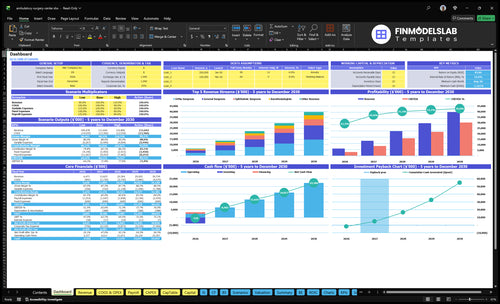
The dashboard shows revenue, staffing, margins, cash flow, and owner take-home; open the Ambulatory Surgery Center Financial Model Template.
Owner-income model highlights
- Owner distribution output
- Revenue and margin bridge
- Case mix and payer mix
Is owning an ambulatory surgery center profitable?
An Ambulatory Surgery Center can be profitable, but not automatically in Year 1. Here’s the quick math: the model shows $350M EBITDA on $647M revenue in Year 1 and $3,079M EBITDA on $3,974M revenue by Year 5, so the business can scale fast if rooms stay full and costs stay controlled.
Profit drivers
- Active operators shape scheduling and staffing.
- Vendor pricing improves with volume.
- Payer follow-up supports cash flow.
- Compliant case flow protects utilization.
Key risks
- Referral dependency can slow volume.
- Payer pressure can cut reimbursement.
- Underused rooms drag margins.
- Debt service and staffing gaps hurt returns.
How do ASC owners get paid?
ASC owners get paid through salary if they work in the Ambulatory Surgery Center, management fees if agreements allow them, and profit distributions after required deductions. For a deeper operating lens, see What Is The Most Important Indicator Of Success For Your Ambulatory Surgery Center?; just remember Year 1 EBITDA of $350M is not the same as cash paid to owners.
Owner pay types
- Pay salary for active work
- Charge fees only if allowed
- Distribute profits after reserves
- Split cash by ownership rights
What controls payout
- Subtract debt before distributions
- Hold taxes and reserves first
- Follow the operating agreement
- Check physician, investor, manager rights
How much revenue does an ambulatory surgery center generate?
An Ambulatory Surgery Center can generate very different revenue based on procedure volume, reimbursement per case, specialty mix, payer contracts, and utilization. In this model, 1,482 billable cases produce $647 million in Year 1, or about $4,366 per case, but that is a model output, not a guaranteed benchmark. Revenue then grows to $2,230 million by Year 3 and $3,974 million by Year 5 as utilization rises from 60% to 65% early to 85% in the mature year.
What drives revenue
- Volume sets the top line.
- Reimbursement changes cash per case.
- Specialty mix affects case value.
- Payer contracts shape pricing power.
Model revenue path
- Year 1: $647 million
- Year 3: $2,230 million
- Year 5: $3,974 million
- Year 1 average: $4,366 per case
Want the six drivers behind ASC owner income?
1
1.5K-8.2KCase Volume
More billable cases spread the fixed lease and staff load; modeled volume rises from 1,482 to 8,160 cases, so this is the biggest profit lever.
2
$1.5K-$8.5KPayer Mix
Year 1 price per case runs from $1,500 in pain to $8,500 in ortho, so contract rates and mix decide revenue per room hour.
3
5 specialtiesSpecialty Mix
Ortho, general surgery, ophthalmology, anesthesia, and pain shift both margin and room use, so the case mix can lift or cap EBITDA.
4
18.5%Labor Control
Medical supplies, implants, billing, and marketing take about 18.5% of revenue in Year 1, and the wage stack is about $1.1M, so tight control protects cash.
5
-$1.17MCash Drag
Build-out and equipment spend push minimum cash to about -$1.168M in Month 8, so debt terms and capex timing can wipe out early profit.
6
83.8%Owner Cash
At 83.8% ROE and a 16-month payback, reserve policy and how much cash stays in the business decide what owners can actually take home.
Ambulatory Surgery Center Core Six Income Drivers
Case Volume and Utilization
Case Volume and Utilization
Utilization is the share of room time that turns into billable cases. In this model, it starts at 60% to 65% by specialty and reaches 85% in Year 5, while billable cases rise from 1,482 in Year 1 to 8,160. With fixed overhead at $690k a year, higher fill rate directly lifts profit, cash flow, and owner pay.
Here’s the quick math: $690k / 1,482 is about $466 per case, but at 8,160 cases it falls to about $85 per case. That’s why capacity limits, block scheduling, turnover time, surgeon availability, and pre-authorization delays matter. More cases only help when staffing and care quality hold.
Improve Case Fill Rate
Track booked cases, billable cases, room-day use, turnover minutes, and pre-auth lag. If a room sits idle, fixed costs stay paid anyway, so margin drops fast. The goal is simple: keep each operating day full without stretching staff or hurting care.
- Measure booked vs. billable cases.
- Watch specialty-by-specialty utilization.
- Cut turnover minutes first.
- Protect surgeon block schedules.
- Flag pre-auth delays weekly.
1
Payer Mix and Reimbursement
Payer Mix and Reimbursement
Payer mix drives what each case actually brings in, not just what gets billed. In Year 1, modeled revenue per billable case ranges from $1,500 for pain physicians to $8,500 for ortho surgeons, with average modeled revenue at about $4,366 per case. At 100 billable cases, that is about $436,600 in modeled revenue.
Commercial contracts, Medicare rates, self-pay terms, out-of-network limits, denials, and collections change cash flow and profit. If the mix skews to lower-paying payers, owner pay drops even when volume holds. This is a modeled revenue assumption, not reimbursement advice, so the real test is collected cash per case, not billed charges.
Track realized cash per case
Measure billed charge, allowed amount, collected amount, and days to cash by specialty and payer. That shows where the margin leaks are. If ortho, commercial, or Medicare cases pay below model, update the case mix forecast fast so the owner sees the hit before draws are set.
Watch denial rate and collection lag every month. A few points of slippage can wipe out the gain from a higher case count. Keep one simple dashboard: cases, average cash per case, denial rate, and net collections. That tells you whether revenue quality is strong enough to support payroll, debt, and owner distributions.
2
Specialty and Procedure Mix
Specialty and Procedure Mix
Mix drives both revenue and cost per case. A modeled ortho case at $8,500 can bring far more cash than pain at $1,500, but ortho can also carry implant exposure and longer room time. The owner’s income follows the weighted margin after supplies, staffing, and room use, not the highest sticker price.
Ophthalmology at $3,500, general surgery at $6,000, and anesthesia at $2,000 can support volume, but each specialty hits margin differently. Here’s the quick math: moving one case from pain to ortho adds $7,000 in billed revenue before added cost, so contract rates and case time decide whether take-home rises.
Track Margin by Specialty
Measure each specialty by price, supplies, staff minutes, implant cost, and room time. The best mix is the one with the highest contribution per OR hour, not the highest charge. If a higher-priced case uses more labor or implants, it can pay less to the owner than a lower-priced case with faster turnover.
- Case count by specialty
- Contract rate per procedure
- Supply and implant cost
- Room minutes and turnover
- Staff time per case
3
Staffing and Supply Cost Control
Staffing and Supply Cost Control
This driver covers supplies, implants, anesthesia support, nurses, surgical techs, sterile processing, and vendor pricing. In the model, medical and surgical supplies are 80% of revenue and implants are 50%, while payroll is $109M in Year 1 and rises to $190M by Year 5. If those ratios creep up, gross margin drops and there is less cash for owner pay.
Understaffing can backfire. With 4 registered nurses, 3 surgical technicians, and 2 sterile processing techs, the center needs enough coverage to keep cases ready and compliant. If staffing is too thin, delays and cancellations can cost more than the wages saved, and that hits revenue, margin, and cash flow fast.
Track cost per case, not just payroll
Measure supplies per case, implant spend, overtime, and cancellation rate by specialty. Compare vendor pricing monthly and watch any procedure where labor time or supply cost rises faster than revenue. The key inputs are case mix, staffing hours, implant use, waste, and turnover time.
Staff to the block schedule, not a guess. Keep a small buffer for safe care and sterile processing, but test whether each extra hour of labor or supply cost is buying more completed cases. If not, it is cutting owner income instead of protecting it.
4
Debt Service and Capex
Debt Service and Capex
Accounting profit can overstate owner cash. The model shows $575k monthly fixed overhead, including $30k lease, $10k insurance, $5k utilities, $4k maintenance, $3k IT, $2k compliance, $25k professional services, and $1k supplies. Any loan payments, equipment financing, or buildout spend comes out after EBITDA, so take-home can drop fast.
EBITDA means earnings before interest, taxes, depreciation, and amortization. If capex and debt values are not in the model, you cannot state owner income with confidence. Working capital also traps cash, especially when payer collections lag, so distributions can trail reported profit by months.
Track cash before draws
Measure monthly debt service, replacement capex, and cash tied in receivables before setting owner pay. The missing inputs are loan balance, interest rate, term, equipment financing, and replacement timing, so any draw forecast stays provisional until they are added.
- Track debt payment dates.
- Reserve for equipment replacement.
- Watch receivable days closely.
- Test draw timing each month.
5
Ownership Share and Reserve Policy
Owner Take-Home Rules
Owner pay is set by equity share, the operating agreement, and when cash is actually distributed. Year 1 EBITDA is $350M before any owner split, but no ownership percent, tax rate, reserve policy, or debt service was supplied, so personal income cannot be stated as a guaranteed amount.
Here’s the quick math: cash for the owner equals EBITDA times the owner’s share, then adjusted for retained cash and timing. Retained earnings may stay in the business for equipment, staff growth, payer delays, compliance work, and expansion, so paper profit can be much higher than take-home.
Control the Distribution Policy
Set a written reserve policy that says what stays in the business and what gets paid out. Track month-end cash, open claims, and planned spending before approving distributions. If the center is holding cash for equipment, staffing, or compliance, owner pay should wait until those needs are covered.
Tie payouts to the operating agreement, not habit. The owner should watch the distribution rate, reserve balance, and cash collections each month so take-home income rises only when the center has real excess cash.
6
Compare lean, base, and high ASC owner-income scenarios
Owner income scenarios
Owner income changes fast with case volume, pricing, staffing, and fixed overhead. These lean, base, and high cases show facility cash flow before debt, taxes, reserves, and owner split.
| Scenario | Lean CaseLean Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Year 1 is the lean opening case with lower utilization and fewer billable cases. | Year 3 is the core operating case with steadier volume and better utilization. | Year 5 is the stronger earnings path with high throughput and tight capacity use. |
| Typical setup | Revenue is $647M with $350M EBITDA, 1,482 modeled billable cases, $109M payroll, and $690k fixed overhead. | Revenue is $2,230M with $1,623M EBITDA, 4,615 modeled billable cases, and a 728% margin. | Revenue is $3,974M with $3,079M EBITDA, 8,160 modeled billable cases, and a 775% margin. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $350MLean Case | $1,623MBase Case | $3,079MHigh Case |
| Best fit | Use this to stress-test opening month ramp, staffing load, and how fast case volume covers fixed overhead. | Use this as the planning anchor for normal operations and mid-cycle owner income. | Use this to test upside if surgeon volume, case mix, and utilization all stay strong. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Ambulatory Surgery Center Porter's Five Forces Analysis
- Ambulatory Surgery Center BCG Matrix
- Ambulatory Surgery Center Business Model Canvas
- 7 Critical Financial KPIs for Your Ambulatory Surgery Center
- Ambulatory Surgery Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Ambulatory Surgery Center Profitability
- Operating Costs: Running an Ambulatory Surgery Center (ASC) in 2026
- Ambulatory Surgery Center Startup Costs: $505M Funding Plan
- Ambulatory Surgery Center Financial Model Template in Excel
- How To Open An Ambulatory Surgery Center In 12 To 24 Months
- How to Write an Ambulatory Surgery Center Business Plan
- Ambulatory Surgery Center Marketing Mix
- Ambulatory Surgery Center Marketing Plan
- Ambulatory Surgery Center Business Proposal
- Ambulatory Surgery Center PESTEL Analysis
- Ambulatory Surgery Center Pitch Deck Example Editable PPTX
- Ambulatory Surgery Center Business SWOT Analysis
- Ambulatory Surgery Center Value Proposition Canvas
Frequently Asked Questions
A passive investor’s income depends on ownership percentage and distributions, not total facility profit This model shows $350M of Year 1 EBITDA on $647M revenue, but debt service, taxes, reserves, and partner terms come first Without an ownership share or distribution policy, personal take-home can’t be calculated responsibly