Ambulatory Surgery Center Startup Costs: $505M Funding Plan

This ASC startup cost breakdown separates $388 million of CAPEX from pre-opening expenses, working capital, and financing needs across the launch period In the model, cash bottoms at -$1168 million in Month 8, so total funding planning is closer to $505 million before excluded financing costs Year 1 EBITDA is $3331 million, but that outcome depends on surgeon volume, payer collections, and a clean opening ramp
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for an ambulatory surgery center, with spending concentrated in Month 1 through Month 9.
CAPEX only This calculator excludes working capital, payroll runway, debt service, owner distributions, deposits, inventory runway, marketing runway, operating expenses, and pre-opening payroll. The model's cash trough is in Month 8, so separate non-CAPEX funding is still needed.
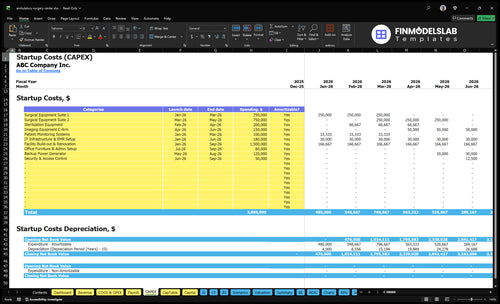
What should the ASC financial model screenshot show?
The Ambulatory Surgery Center Financial Model Template screenshot should show CAPEX, startup costs, launch timing, and depreciation/amortization. Review assumptions.
Key screenshot highlights
- CAPEX tab totals $388M
- Month 1 to 9 timing
- Month 8 cash trough
How much funding do you need to open an ambulatory surgery center?
You need roughly $5.05M before financing costs to open an Ambulatory Surgery Center: $3.88M in CAPEX plus a $1.168M Month 8 cash deficit; for the operating metric that matters after launch, see What Is The Most Important Indicator Of Success For Your Ambulatory Surgery Center?. That is opening cash, while $3.331M Year 1 EBITDA and a 16-month payback are model outputs after ramp-up.
Opening cash
- Fund $3.88M CAPEX
- Cover $1.168M Month 8 deficit
- Plan CAPEX from Month 1 to Month 9
- Include $1.085M Year 1 payroll
Cost drivers
- Lease: $30k per month
- Insurance: $10k per month
- IT subscriptions: $3k per month
- Adjust for payer timing, accreditation, OR count, specialty mix, and contingency
How should an ambulatory surgery center funding plan be built?
Build the Ambulatory Surgery Center funding plan around lender-testable assumptions, not just a growth story. Tie the $388M CAPEX schedule to the $1,168M cash trough, launch timing, OR capacity, payer mix, reimbursement, staffing, supply cost, implant cost, and collections lag. Use Year 1 capacity of 600% for orthopedic, general surgery, and anesthesia, and 650% for ophthalmic and pain, plus Year 1 prices of $8,500, $6,000, $3,500, $2,000, and $1,500.
Debt and equity
- Size debt to the cash trough.
- Match draws to launch timing.
- Test covenant headroom early.
- Hold a working capital reserve.
Operating inputs
- Set OR capacity by specialty.
- Use specialty price assumptions.
- Stress payer mix and reimbursement.
- Model staffing, supply, and implant costs.
What are the biggest cost drivers for an ambulatory surgery center?
The biggest cost drivers for an Ambulatory Surgery Center are the facility build-out and the surgical equipment base. A base case can start at $15M for build-out and $15M for two surgical equipment suites, before adding $200k sterilization equipment, $150k C-arm imaging, $120k backup generator, $100k patient monitoring, and $180k IT infrastructure. Costs then move with the number of operating rooms, specialty mix, anesthesia coverage, sterile processing needs, local code, medical gas, HVAC, life safety, and leased shell condition.
Capital spend drivers
- $15M build-out baseline
- $15M for two suites
- $200k sterilization equipment
- $150k C-arm imaging
Volume and scope drivers
- More rooms raise total cost
- Orthopedics needs more instruments
- Each specialty adds trays and storage
- General surgery and pain change setup
Calculate Fuding Needs
Startup cost summary
This table summarizes ambulatory surgery center startup assets and the excluded launch cash need across low, base, and high cases.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Facility Build-out & Renovation | $1,500,000 | Space build and clinical room fit-out | Yes |
| Surgical Equipment Suite 1 | $750,000 | One operating room equipment package | Yes |
| Surgical Equipment Suite 2 | $750,000 | Second operating room equipment package | Yes |
| Sterilization Equipment | $200,000 | Sterile processing and instrument prep | Yes |
| IT Infrastructure & EMR Setup | $180,000 | Systems, network, and records setup | Yes |
| Working Capital Runway | $1,168,000 | Month 8 cash trough and startup operating losses | No |
Ambulatory Surgery Center Core Five Startup Costs
Facility Build-Out & Renovation Startup Expense
Base Build-Out
The base case uses $15M from Month 1 through Month 9 to build the ASC shell-out: operating rooms, procedure rooms, PACU and recovery bays, sterile corridors, HVAC, medical gas, plumbing, electrical, emergency power tie-ins, accessibility, infection-control finishes, life safety, nurse stations, med rooms, and storage. Here’s the quick math: budget is driven by the full clinical fit-out, not just square footage.
Cost Drivers
Estimate this line from the leased-space condition, OR count, specialty mix, local code, inspection findings, and the landlord work letter. A cleaner shell lowers spend; a rough shell pushes it up. One line to keep in mind: the more code fixes and specialty build requirements you have, the slower the schedule and the bigger the check.
- Check shell and utility condition first
- Map costs by room type
- Review code gaps early
What To Exclude
Keep landlord-funded tenant improvements separate from the rest of the startup budget. This build-out bucket should not carry medical equipment, software, licensing, or pre-opening staffing. Put each excluded item in its own line so the facility number stays clean, the landlord scope stays clear, and you can compare bids without mixing construction with operating launch costs.
Timing And Contingency
Plan cash to flow across the full 9-month build window, not front-loaded in month one. Hold a separate contingency line for inspection findings and landlord scope gaps, since those items can move fast and cost real money. If the work letter is narrow, expect more out-of-pocket capex from the tenant side.
Medical Equipment & Surgical Assets Startup Expense
Base Cost
For a two-suite ambulatory surgery center, the base equipment package is about $1.95 million: two surgical suites at $750k each, sterilization gear at $200k, a C-arm at $150k, and patient monitoring at $100k. Add $4k per month after launch for maintenance contracts. This is separate from build-out and working capital.
What It Covers
The suite budget covers surgical tables, lights, anesthesia machines, monitors, specialty scopes or instruments, autoclaves, sterilizers, crash carts, instrument sets, and recovery gear. To estimate it, use suite count × vendor quote, then add service terms and delivery. Keep reusable capital equipment separate from disposables, implants, and drugs so case cost stays clean.
- Match gear to specialty mix.
- Use surgeon preference cards.
- Stress-test case volume.
How To Trim It
New equipment costs more, but used gear only works if it is serviceable and compliant. Real savings come from not buying tools surgeons won’t use and from limiting maintenance to high-failure items. The main cost drivers are specialty mix, surgeon preference, and case volume, so reprice the package when those inputs change.
Main Cost Drivers
A center built for orthopedics or gastroenterology may need different scopes, instruments, and recovery sets than pain management. That’s why the spend should be rebuilt from actual surgeon use, not a generic list. Requote when the specialty mix changes, because the equipment buy and the $4k monthly service load move with it.
Licensing, Accreditation & Certification Startup Expense
What it covers
Licensing and accreditation for an ASC usually includes state licensure, accreditation readiness, Medicare certification planning through the Centers for Medicare & Medicaid Services, policy and procedure work, life-safety reviews, infection-control documentation, legal support, and certificate-of-need review where required. The base model carries $2k per month in regulatory compliance and licensing, but state rules and payer strategy can change the total fast.
Cost buckets
Build this line as filing fees + consultant support + readiness labor + inspection fixes + recurring compliance. Use state fee schedules, consultant quotes, staff hours, and the punch list from surveys to size it. The recurring piece is the clearest number here: $2k per month for compliance and licensing.
- Separate one-time and monthly costs
- Price fixes from survey findings
- Use quotes, not guesses
Keep it clean
Front-load policy writing, infection-control files, and life-safety prep before the survey so you do the work once. Get a gap review early, and don’t skip legal help if certificate-of-need review applies. That usually saves more than it costs, while keeping quality and compliance intact.
Recurring load
After launch, keep $2k per month in the budget for regulatory compliance and licensing. It is a small line next to build-out, but it still needs an owner for renewals, policy updates, and survey prep. Track it as recurring overhead, not a one-time setup cost.
Software, EMR & Administrative Systems Startup Expense
Setup Cash
If you’re opening an ambulatory surgery center, the base case puts $180k into IT infrastructure and EMR setup across Months 1-6, plus $3k per month for software and IT subscriptions. That cash is needed before steady case volume starts, so it belongs in startup funding, not just operating expense.
What It Covers
This bucket includes ASC management software, scheduling, billing, revenue cycle management, clearinghouse setup, patient communications, cybersecurity, phones, networking, document storage, compliance logs, and reporting. Split one-time implementation, hardware, data migration, training, and interfaces from recurring subscriptions so the budget stays clean.
- Separate setup from monthly fees.
- Count every interface upfront.
- Quote training before go-live.
Build The Estimate
Build the estimate from vendor quotes, seat counts, interface needs, and months of coverage. Here’s the quick math: $180k setup plus $3k monthly means $216k if you carry a full year of subscriptions. Billing setup matters too, because Year 1 billing and collections fees run at 35% of revenue.
Keep It Lean
Buy only the interfaces you need at launch, delay nonessential add-ons, and train staff before go-live. What this estimate hides is the cost of bad data migration and claim rework; if those are weak, cash gets squeezed fast even when the software price looks low.
Pre-Opening Staffing, Supplies & Working Capital Startup Expense
Staffing Runway
For an ambulatory surgery center, this bucket is pre-opening expense plus working capital, not facility CAPEX. Year 1 payroll is about $10.85M, or $904k per month, for the administrator, clinical director, registered nurses, surgical technicians, sterile processing techs, front desk admissions, billing, and medical records support.
Fixed Cash Load
Base monthly fixed costs are $575k before payroll. Add $10k per month for insurance premiums, plus initial disposables, drugs, implants, credentialing support, marketing, and payer setup. Here’s the quick math: monthly burn is roughly $1.49M before variable case supplies, so plan cash by months of runway, not just launch spend.
Working Capital Need
Working capital should cover the Month 8 minimum cash deficit of -$1.168M and slow collections. That means enough cash to pay staff and vendors before revenue clears. If payer setup or claims lag, the deficit gets worse, so the reserve needs to sit inside startup funding, not on the operating line.
Spend Control
Keep this spend tight by hiring to case ramp, staging credentialing early, and buying initial supplies in small lots. Tie payroll starts to open-date milestones and payer approval timing. The main mistake is underfunding collections lag; even a fully staffed center can run short if cash does not cover the first months of claims delay.
Compare 3 Startup Cost Scenarios
Scenario Table
More ORs, more specialties, and heavier build-out push startup cost fast in an ambulatory surgery center. Lean trims rooms, equipment, and staffing; full adds capacity, recovery space, and cash reserve.
| Scenario | Lean LaunchLowest build risk | Base LaunchBalanced plan | Full LaunchHighest capacity |
|---|---|---|---|
| Launch model | Single-specialty leased-space launch with fewer rooms, lighter equipment, and tighter staffing. | Two-suite multi-specialty launch using the modeled case mix and staffing ramp. | Multi-specialty launch with more ORs, heavier imaging, stronger sterilization, and a larger launch reserve. |
| Typical setup | One or two ORs, narrow specialty mix, limited recovery space, and lower working capital. | Two surgical equipment suites, $1.5M build-out, standard EMR setup, and full support staff. | More rooms, broader orthopedic mix, bigger recovery flow, and a larger staffing model. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | Below base caseLower funding need | $3.88M - $5.05MCore funding band | Above base caseHighest funding need |
| Best fit | Best for founders testing one specialty before a broader rollout. | Best for operators using the researched model as the main financing plan. | Best for teams planning a full-scale center with higher volume and more launch complexity. |
Planning note: Scenario ranges are researched planning assumptions, not exact quotes or bids.
Related Products
- Ambulatory Surgery Center Porter's Five Forces Analysis
- Ambulatory Surgery Center BCG Matrix
- Ambulatory Surgery Center Business Model Canvas
- 7 Critical Financial KPIs for Your Ambulatory Surgery Center
- Ambulatory Surgery Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Ambulatory Surgery Center Profitability
- Operating Costs: Running an Ambulatory Surgery Center (ASC) in 2026
- Ambulatory Surgery Center Financial Model Template in Excel
- How Much Does an ASC Owner Make? $35M First-Year Cash Flow
- How To Open An Ambulatory Surgery Center In 12 To 24 Months
- How to Write an Ambulatory Surgery Center Business Plan
- Ambulatory Surgery Center Marketing Mix
- Ambulatory Surgery Center Marketing Plan
- Ambulatory Surgery Center Business Proposal
- Ambulatory Surgery Center PESTEL Analysis
- Ambulatory Surgery Center Pitch Deck Example Editable PPTX
- Ambulatory Surgery Center Business SWOT Analysis
- Ambulatory Surgery Center Value Proposition Canvas
Frequently Asked Questions
The researched base case needs about $505 million before financing costs That comes from $388 million of CAPEX plus a $1168 million cash trough in Month 8 The largest CAPEX items are $15 million for build-out and $15 million for two surgical equipment suites