 Time to Open8-16 weeksOpening prep
Time to Open8-16 weeksOpening prepHow To Open An Assistive Technology Assessment Service In 8–16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8-16 weeksOpening prep  Launch Sequence5 stagesCredentials first
Launch Sequence5 stagesCredentials first Key BottleneckTrust gateScope clarity
Key BottleneckTrust gateScope clarity First Revenue StepPaid evalPrivate booking
First Revenue StepPaid evalPrivate booking


You’re launching a credential-dependent assistive technology (AT) assessment service, so the work starts with scope, privacy, documentation, referral trust, and first-client workflow This guide covers the opening sequence over a typical 8 to 16 week launch window, with Year 1 planning assumptions of 6 specialists, about 42 capacity-adjusted assessments per month, and a practical next step: validate your service scope before taking clients
Time to Open8-16 weeksOpening prepLaunch Sequence5 stagesCredentials firstKey BottleneckTrust gateScope clarityFirst Revenue StepPaid evalPrivate bookingLaunch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Credentials and compliance
- Verify credentials
- Check licensure scope
- Build HIPAA workflow
- Approve consent forms
- Clear marketing claims
Service design
- Map assessment scope
- Define service tiers
- Draft intake forms
- Set report template
Tools and vendors
- Demo devices
- Compare vendor quotes
- Confirm access terms
- Order starter kits
Operations setup
- Set scheduling flow
- Configure invoicing
- Set payer contracts
- Test intake flow
Referral outreach
- Draft referral scripts
- Build outreach list
- Start partner outreach
- Share launch packet
Pilot launch
- Screen pilot clients
- Run pilot visits
- Test turnaround times
- Review pilot feedback
- Go-live decision
Why test launch assumptions before you open?
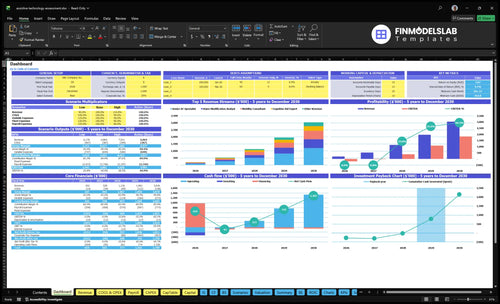
If you're launching Assistive Technology Assessment Service, this Assistive Technology Assessment Service Financial Model Template is a validation tool: it checks launch timing, volume, referrals, staffing, cash runway, pricing, and break-even. Year 1 starts with 6 specialists, 417 capacity-adjusted assessments a month, and about $16,795 monthly revenue.
Financial model highlights
- Launch timing
- Assessment volume
- Cash runway
- Staffing capacity
- Break-even path
What are common mistakes opening an assistive technology assessment service?
The biggest mistakes opening an Assistive Technology Assessment Service are fuzzy scope, weak records, no referral base, and pricing that ignores payment terms. In year 1, if travel and in-home visits eat 60% of revenue and referral commissions take 50%, sloppy routing can crush contribution fast. Fix it with state-specific credential review, intake-to-follow-up templates, partner outreach before launch, and strict scheduling, travel-radius, and report-turnaround rules.
Common launch errors
- Unclear scope slows sales.
- Weak documentation raises risk.
- No referral pipeline delays demand.
- Poor privacy can break trust.
Launch fixes
- Review state credentials before opening.
- Use intake, consent, and follow-up templates.
- Build partner outreach before month one.
- Set payment terms and report rules.
What credentials are needed to start an assistive technology assessment service?
Credentials for an Assistive Technology Assessment Service depend on scope: clinical work may require state-licensed clinicians, while consulting work may rely on qualified assessors or Assistive Technology Professional credential holders. Treat licensure as a launch dependency before pricing, claims, or intake; for the money side, see How Increase Profitability Of Assistive Technology Assessment Service?.
Credential checks
- Verify state licensure by service line
- Check occupational therapy rules in 50 states
- Use ATP where payer expects it
- BLS: OT median pay was $96,370
Launch sequence
- Define scope first: clinical, school, vocational
- Check credentials second, before claims
- Write intake rules around assessor limits
- Plan 5 Year 1 specialist roles
How do you get clients for an assistive technology assessment service?
Get clients for an Assistive Technology Assessment Service by starting with referral sources, not broad ads: occupational therapists, rehab clinics, special education teams, aging-in-place providers, vocational rehabilitation counselors, disability nonprofits, case managers, senior-care providers, and private-pay families. Lead with your qualified scope, report format, turnaround, pricing, and how referrals are handled; that’s what builds trust fast. For a quick read on pricing and margin setup, see How Increase Profitability Of Assistive Technology Assessment Service? First revenue can come from a paid private assessment or a referral-based evaluation contract, with Year 1 prices of $450 for Senior AT Specialist assessments, $350 for mobility, $300 for cognitive aid, $300 for vision support, and $550 for home modification analysis.
Referral First
- Start with occupational therapists
- Reach rehab clinics first
- Call special education teams
- Ask aging-in-place providers
Trust Fast
- Explain qualified scope clearly
- Share sample report sections
- State turnaround expectations
- List follow-up steps up front
Confirm what must be ready before serving AT assessment clients
Launch readiness checklist
Use this go-live approval checklist to confirm the service is ready before opening.
Scope
- Service scope approvedCritical
Block launch if the service scope is vague or outside your qualified assessment work.
- State licensure checkedCritical
Confirm the launch state allows these services before any client booking.
- Clinical credentials verifiedCritical
ATP or clinical proof keeps the team inside a safe, qualified scope.
- Insurance coverage boundHigh
Coverage should be active before any home visit, consult, or report.
Privacy
- Signed consent formsCritical
No signed consent means no assessment, simple as that.
- HIPAA privacy workflowCritical
Set how records, photos, and notes move so client data stays private.
- Intake forms approvedHigh
Standard intake cuts rework and gives the assessor usable history.
Workflow
- Assessment template finalizedHigh
Use one template so every evaluator covers the same key questions.
- Evaluation report format approvedHigh
Clients and referral partners need a clear report they can act on.
- Follow-up rules setMedium
Define when to call back, close the loop, and refer out.
Delivery
- Travel radius setHigh
A fixed radius keeps visit time, cost, and scheduling realistic.
- Telehealth limits setMedium
Required if any consults happen remotely.
- Scheduling rules approvedHigh
Set visit length, buffers, and no-show rules before booking starts.
Equipment
- Vendor sourcing confirmedHigh
Lock core device and resource sources before the first assessment.
- Demo inventory readyHigh
You need working sample devices to test fit, use, and recommendations.
- Mobile kit packedMedium
Field visits stall fast if tablets, tools, or forms are missing.
- Records software testedCritical
Test booking, notes, and records flow before live client work.
Commercial
- Referral outreach readyCritical
Launch needs a referral source before day one or demand stays thin.
- Pricing and invoicing setCritical
Prices should match the $300 to $550 plan and bill cleanly.
- Payment flow testedCritical
If clients cannot pay or be billed, revenue stops at intake.
- Cash runway confirmedCritical
The model bottoms out at month 24 with $563k minimum cash.
- Go-live signoff completeCritical
Do not open until scope, privacy, workflow, and revenue steps are green.
Which launch drivers matter most before opening?
1Qualified Scope
License gateWritten scope and credential checks must clear first, or marketing and intake can't start.
2Assessment Workflow
1 reportA repeatable assessment report keeps recommendations consistent and cuts rework after the first visit.
3Referral Pipeline
10/wk rampTrusted referral sources must feed about 10 assessments a week once ramp starts.
4Vendor Ecosystem
Demo listCurrent device and vendor data keeps recommendations usable and avoids quote delays.
5Service Logistics
60% travelTight scheduling and travel rules protect capacity, since in-home visits drive most variable cost.
6Pricing Ops
$300-$550Clear rates and billing steps decide who pays, when cash comes in, and whether launch stays funded.
Qualified Scope, Credentials, And Compliance
Scope and Credentials Gate
This is the launch gate before marketing or intake. If the service cannot clearly say what it can assess, who can perform each evaluation, and where the rules change by client type, opening slips and day-one work gets risky.
For this model, the written scope has to cover clinical, school, vocational, and private-pay clients. The team plan includes 2 Senior AT Specialists, 1 Mobility Consultant, 1 Cognitive Aid Expert, 1 Vision Support Specialist, and 1 Home Modification Analyst, so each role needs a state-checked credential file before referral outreach starts.
Verify Scope Before Selling
Build a service-line matrix first: what each role can assess, what licensure or credential proof is on file, and what consent and privacy language applies. Then review claims so the website, referral sheet, and intake form match the legal scope. One clean rule: no outreach before qualification is documented.
- Review state licensure and limits
- File credential documents by role
- Approve consent and privacy workflow
- Check every service claim
- Separate clinical and nonclinical scope
What this controls is first-day trust. If a client expects a clinical-style evaluation and the assessor is not qualified for that scope, the business risks rework, delayed intake, and a bad referral loop before the first invoice.
1
Assessment Workflow And Documentation
Repeatable Assessment Workflow
The report is the product, so opening on time depends on a repeatable workflow from inquiry to follow-up. If intake, consent, needs review, device comparison, and recommendation logic are not standardized, the first clients will get slow turnarounds and inconsistent reports, which can stall referrals and trigger rework calls.
The key dependency is privacy workflow before collecting client information. Day-one readiness means the team can move from intake to a clear report format across mobility, cognitive aid, vision support, and home modification services without guessing what to ask, document, or deliver.
Lock the Report Template Before Launch
Build one shared workflow for intake forms, consent, needs assessment, environment review, device comparison, recommendation logic, implementation notes, quote requests, and follow-up steps. Then test it on a mock case so you can see where notes, approvals, or handoffs slow down. That tells you whether the launch team can finish a report fast enough to support first-week revenue.
Verify the minimum inputs before the first appointment: client goals, setting, current tools, barriers, and any privacy consent needed to store or share data. If the process is loose, reports will vary by assessor, which hurts trust with families, schools, and agencies and makes the business look unready even if the assessment itself is strong.
- Use one report format everywhere
- Test privacy before intake starts
- Standardize quote requests early
- Assign follow-up tasks by role
2
Referral Pipeline Readiness
Trusted Referral List Before Opening
Launch depends on warm trust, not broad awareness. If the first named outreach list is weak, opening week can start with empty calendars, slow cash inflow, and more time spent chasing leads than serving clients. The core gate is simple: clinicians, schools, case managers, disability groups, senior-care providers, vocational rehab contacts, and private-pay decision makers need a clear reason to refer before month one.
Here’s the quick math: the Year 1 model assumes 417 capacity-adjusted monthly assessments, or about 10 assessments per week once ramped. That means referral flow has to be real on day one, not “we’ll post on social media and see.” One clean one-liner: no trusted referrals, no reliable launch.
Build the referral engine first
Before opening, verify the outreach list, the referral explanation, and the first assessment offer. The founder should finish partner calls, a sample report outline, a pricing sheet, a referral intake process, and a follow-up cadence so every contact gets the same answer on scope, timing, and next step.
- Use qualified scope before outreach.
- Show one clear first assessment offer.
- Track follow-ups within set days.
- Avoid generic social media dependence.
What this hides: if the referral message is vague, partners may wait, send the wrong cases, or hold back until they trust the documentation. That slows first revenue and can push the business past its planned opening date.
3
Vendor And Technology Ecosystem
Vendor and Demo Readiness
Opening depends on knowing which assistive tools you can recommend today, not just what exists in the market. For each assessment type, you need current vendor contacts, trial access, quote steps, and installer leads for communication tools, mobility aids, vision supports, cognitive aids, and home accessibility options.
The risk is simple: stale pricing or no setup help slows reports and weakens client trust. If a recommendation cannot be quoted, tested, or installed in a realistic time frame, the assessment may still look complete on paper but fail on day one. The vendor file is part of the service, not an extra.
Build the vendor matrix before intake
Start with a vendor and demo list by assessment type, not a large inventory room. For each category, record the device class, quote path, trial process, local installer contact, and the date the pricing or availability was checked. Add a vendor independence policy so the report stays client-first and free of biased product pushing.
- Check pricing before first report
- Confirm at least one trial path
- Verify local install support
- Log refresh dates by category
Test the full path before opening: request one quote, line up one demo, and confirm one implementation contact for each major service line. If any step takes too long or breaks, fix it before launch. That keeps report turnaround tight and avoids first-client delays when a tool has to move from recommendation to real use.
4
Service Delivery Logistics
Scheduling, Travel, And Day-One Flow
Service delivery logistics decides whether the business can start on time or gets stuck in reschedules, missing files, and unclear visit rules. For this service, the first inquiry has to move cleanly into intake, consent, and a completed assessment, or the launch slips fast. Privacy and consent must be in place before any assessment notes are taken.
Here’s the pressure point: Year 1 travel and in-home visit costs are modeled at 60% of revenue, and role utilization ranges from 500% to 650%, so route planning and calendar control shape capacity from day one. If travel radius, telehealth limits, or accessibility needs are not written down, each visit can create delay, extra admin, and lower first-month revenue.
Lock The Operating Rules Before First Booking
Set the workflow before opening: schedule setup, intake triage, travel radius, in-home visit rules, telehealth limits, accessibility screening, documentation turnaround, follow-up tasks, and report delivery. That gives staff one path from inquiry to completed assessment and cuts back-and-forth with clients, caregivers, and referral sources.
- Write the intake and consent steps first.
- Map routes before opening the calendar.
- Set report deadlines and file storage rules.
- Test reminder texts and follow-up handoffs.
- Limit travel zones to protect capacity.
A practical check: if a visit needs drive time, secure files, and a report turnaround window, confirm those steps can still fit the week without pushing assessments out. If not, opening day starts with a backlog instead of completed work.
5
Pricing, Payer, And Revenue Operations
Pricing and Cash Setup
This launch driver decides who pays, when they pay, and whether the business can open without cash gaps. A pricing sheet tied to service type has to exist before the first appointment, because $450 Senior AT Specialist, $350 mobility, $300 cognitive aid, $300 vision support, and $550 home modification analysis all carry different billing and contract rules.
If pricing, invoices, and payment terms are not set, the team can still do assessments but won’t know how fast cash comes in. That creates a real launch risk with agency, school, private-pay, and insurance billing paths. The bottleneck is simple: service scope comes before pricing, or you end up delivering work before you know who pays and when.
Lock Payment Workflow First
Before opening, verify the rate card, invoice template, deposit or payment policy, contract terms, payer feasibility review, and revenue tracking. The workflow should be ready before first appointment, not after the first report is sent.
- Match each service to one rate.
- Test invoicing before launch.
- Set payment timing in writing.
- Check insurance billing feasibility early.
- Track revenue by service type.
One clean rule helps: no assessment starts without a clear payer path. If the business opens with only service prices but no payment process, collections slip, staff lose time chasing invoices, and early revenue ramps slower than planned.
6
Related Products
- Assistive Technology Assessment Service Porter's Five Forces Analysis
- Assistive Technology Assessment Service BCG Matrix
- Assistive Technology Assessment Service Business Model Canvas
- What 5 KPIs For Assistive Technology Assessment Service Business?
- Assistive Technology Assessment Service Business Plan Template in Pre-Written Word
- How Increase Profitability Of Assistive Technology Assessment Service?
- What Are Operating Costs For Assistive Technology Assessment Service?
- Assistive Technology Assessment Startup Costs: $116k Monthly Overhead
- Assistive Technology Assessment Financial Model Template in Excel
- How Much AT Assessment Owners Make: $26K To $247M Before Pay
- How To Write A Business Plan For Assistive Technology Assessment Service?
- Assistive Technology Assessment Service Marketing Mix
- Assistive Technology Assessment Service Marketing Plan
- Assistive Technology Assessment Service Business Proposal
- Assistive Technology Assessment Service PESTEL Analysis
- Assistive Technology Assessment Service Pitch Deck Example Editable PPTX
- Assistive Technology Assessment Service Business SWOT Analysis
- Assistive Technology Assessment Service Value Proposition Canvas
Frequently Asked Questions
Start by defining your qualified scope, then build intake, consent, privacy, assessment, report, referral, and billing workflows The planning case uses an 8 to 16 week launch window, 6 Year 1 specialists, and about 42 capacity-adjusted assessments per month Don’t sell services before credential and state-specific scope checks are complete