 Owner income-$193k to $1.83M
Owner income-$193k to $1.83MHow Much AT Assessment Owners Make: $26K To $247M Before Pay

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income-$193k to $1.83M  Net margin-96% to 60%
Net margin-96% to 60% Revenue for target pay$1.14M
Revenue for target pay$1.14M Business difficultyHard
Business difficultyHard


An assistive technology assessment owner can’t treat revenue as take-home pay Using the researched assumptions, the business produces about $26k in operating cash before owner salary in Year 1, after listed direct costs and $1392k of fixed overhead The model includes a $145k CEO and Clinical Director salary, so Year 1 does not support that full pay from listed operations alone By Year 2, revenue reaches about $5285k and can support the $145k salary before unprovided payroll, taxes, debt, and reserves
Owner income-$193k to $1.83MNet margin-96% to 60%Revenue for target pay$1.14MBusiness difficultyHardWhat owner income do your assumptions support?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual take-home changes with revenue mix, payroll, taxes, debt, and reinvestment.
How do you check owner income in the financial model?
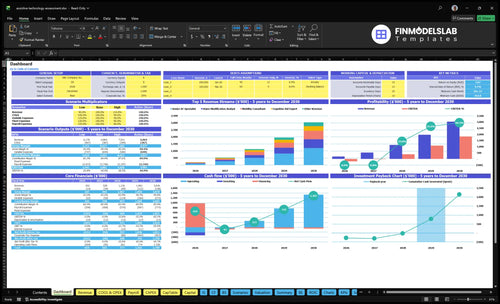
Shows revenue, gross margin, operating profit, salary coverage, and cash runway; open the Assistive Technology Assessment Service Financial Model Template.
Owner-income model highlights
- Owner take-home stays visible.
- Test providers, pricing, capacity, overhead.
- Y1 $2015k; Y3 $114M; Y5 $304M.
How do you scale an assistive technology assessment service?
Scale comes from more qualified assessors, better referral channels, and steadier contracts with schools, agencies, vocational rehabilitation programs, healthcare sources, and private-pay clients. In the model, providers grow from 6 in Year 1 to 32 in Year 5, and revenue rises from $2,015k to $304M as capacity improves. The catch is that staffed delivery can cut per-assessment margin once subcontractor or employee pay is added, so the owner shifts from assessor to clinical director, scheduler, contract manager, and quality reviewer.
Scale drivers
- 6 providers in Year 1
- 32 providers in Year 5
- Use school and agency referrals
- Keep private-pay demand steady
Margin tradeoff
- Staff pay lowers per-assessment margin
- Subcontractors add direct cost
- Owner becomes quality reviewer
- Owner also manages scheduling
How many assistive technology assessments pay the owner?
To cover the $145k CEO and Clinical Director salary, $1.392m in fixed overhead, and 180% Year 1 direct costs, the Assistive Technology Assessment Service needs about $3.466m in Year 1 revenue before reserves and unlisted payroll. At a blended collected fee of about $407 per completed assessment, that works out to roughly 852 paid assessments a year, or about 71 a month. Collection delays and admin help push the needed volume higher.
Year 1 revenue math
- $3.466m revenue target
- $407 per assessment
- 852 paid assessments yearly
- 71 paid assessments monthly
What raises the target
- Collection delays slow cash
- Admin help adds overhead
- Unlisted payroll is not included
- Reserves sit above this floor
What costs reduce assistive technology assessment profit margin?
The biggest margin hits in an Assistive Technology Assessment Service come from direct service costs first, then fixed overhead. The fastest leaks are 45% on assessment tools and consumables in Year 1, 25% on external lab and test fees, 60% on travel and in-home visits, and 50% on referral commissions; see How Increase Profitability Of Assistive Technology Assessment Service? for the margin-side fix. After that, rent at $45k per month, insurance at $12k, marketing at $30k, continuing education at $15k, software at $800, and utilities at $600 cut operating profit before owner take-home, reserves, and any unlisted staff costs.
Direct cost drains
- 45% on tools and consumables
- 25% on lab and test fees
- 60% on travel and home visits
- 50% on referral commissions
Fixed overhead pressure
- Rent: $45k per month
- Insurance: $12k
- Marketing: $30k
- Continuing education: $15k
What drives owner income most?
1
55-94/moPaid Assessments
More paid assessments per month is the fastest way to spread fixed overhead and lift owner take-home.
2
$300-$640Assessment Fee
A higher collected fee per assessment raises owner take-home without adding the same amount of labor.
3
4%-5%Payer Mix
Better payer and referral mix trims commission drag, so more billed dollars become owner take-home.
4
50%-88%Billable Time
Less report and admin time turns the same staff hours into more billable work and higher owner take-home.
5
3.5-8 FTEStaffing Mix
A leaner staffing mix protects margin as revenue scales, which keeps owner take-home from getting squeezed.
6
$116K/moOverhead
Holding fixed overhead near $116K a month and keeping reserves tight decides how much cash is left for owner take-home.
Assistive Technology Assessment Service Core Six Income Drivers
Completed Paid Assessments
Completed Paid Assessments
This driver matters most because revenue starts with completed and collected assessments, not inquiries. The model’s Year 1 volume comes from 2 Senior AT Specialists, 1 Mobility Consultant, 1 Cognitive Aid Expert, 1 Vision Support Specialist, and 1 Home Modification Analyst, operating at 500% to 650% capacity. If a case is not finished, billed, and collected, it does not reach owner income.
Here’s the quick math: more completed cases raise monthly revenue, but only if referral flow stays steady and reports move out on time. The main leak points are referral gaps, no-shows, travel time, and delayed reports. By Year 5, capacity improves to 850% to 880%, so the owner’s take-home depends on turning that added workload into paid, closed cases instead of unpaid activity.
Track Completion, Not Just Leads
Measure scheduled assessments, completed assessments, billed assessments, and collected assessments every month. That tells you where revenue is leaking. Also track no-show rate, average travel time, and days from visit to report delivery, because those three items directly cut capacity and delay cash.
Use a simple rule: if completion or collection slips, owner income slips with it. Tighten intake, confirm appointments, route visits by geography, and push report templates so work closes faster. The goal is not more activity; it is more finished, billed work that turns into cash.
- Track completed-to-scheduled rate.
- Track billed-to-collected rate.
- Cut no-shows with confirmation calls.
- Reduce travel with smarter routing.
- Speed reports with standard templates.
1
Average Collected Fee
Average Collected Fee
Average collected fee is the cash you actually keep per completed assessment after discounts, denials, and unpaid work. In Year 1, fees run from $300 for cognitive aid or vision support work to $550 for home modification analysis; by Year 5, the range is $360 to $640. A move from $300 to $550 is an 83% lift in collected revenue per case before overhead.
Price drives owner pay. Every $50 increase per completed case adds $50 to gross revenue, so fee setting should match complexity, report depth, travel, payer rules, and specialist skill. If the quoted price looks strong but collections are weak, cash flow and profit still sag.
Price to what you collect
Track realized fee as total cash collected divided by completed assessments. Use it by case type, payer, and specialist, then compare it with travel time, report time, and unpaid follow-up. If denials or discounts rise, owner draw drops even when the schedule looks full.
- Measure cash per completed case.
- Split by complexity and payer.
- Watch denials and write-offs.
- Raise fees on harder cases.
2
Payer And Referral Mix
Payer and Referral Mix
Payer and referral mix is the split between school, agency, vocational rehabilitation, healthcare, and private-pay referrals. It changes volume quality, paperwork, and cash timing. In Year 1, referral commissions are modeled at 50% of revenue, so a $1,000 case keeps only $500 before labor and overhead.
By Year 5, the commission load falls to 40%, which helps margin, but high-volume contracts can still pay slowly or at lower realized fees. Private-pay usually collects faster, but it needs clearer scope and local trust. One clean rule: mix drives cash, not just bookings.
Track source, fee, and days to cash
Measure assessments by source, collected fee, commission rate, and days to collect. Also track paperwork hours by channel, since school and healthcare referrals often add more reporting than private-pay. The real test is contribution after referral share, not booked appointments. If one source fills the calendar but cuts realized fee, it may not improve owner pay.
Use source-level pricing and scope rules. For each channel, test whether the fee covers documentation time, travel, and the referral commission. If private-pay volume is weak, build local trust and make the report package easy to understand. If contract work dominates, negotiate payment timing so cash does not lag behind payroll and fixed overhead.
3
Documentation And Nonbillable Time
Documentation and Nonbillable Time
Report writing, scheduling, travel, coordination, and follow-up are unpaid hours that still use staff time. In this service, fewer nonbillable hours mean more completed paid assessments, faster cash collection, and better owner take-home. The model’s service-line capacity rises from 500% to 650% in Year 1 to 850% to 880% in Year 5, so documentation speed is a direct profit lever.
What this hides is quality risk: cutting clinical detail can create rework. The better move is to shorten report scope, standardize intake forms, use templates, and tighten follow-up rules. Track hours per assessment, travel time, and time from visit to final report, because those inputs drive capacity, revenue timing, and the owner’s ability to pay themselves.
Cut Unpaid Hours
Measure nonbillable hours per assessment and break them into report writing, travel, scheduling, and admin. Here’s the quick math: if those hours fall, each practitioner can finish more assessments without adding headcount, so revenue grows faster than fixed pay. Keep the clinical standard intact, but make the workflow lean.
Use shorter templates, pre-filled intake forms, route planning, and clear follow-up rules. Also track the lag from visit to submitted report; that lag ties up capacity and delays billing. If documentation stays slow, you may still be busy while owner cash flow stays weak.
4
Labor Model And Staffing
Staffing Load
Owner income changes fast when the owner is still delivering assessments versus supervising contractors, hiring employees, or paying admin help. The model scales providers from 6 in Year 1 to 32 in Year 5, so revenue can rise, but profit per assessment can fall if labor costs grow faster than collected fees.
The only disclosed salary is $145k for the CEO and Clinical Director, so owner pay depends on whether that role is paid inside the business or taken as draw. One clean rule: more staff can buy capacity, but it does not guarantee more take-home cash.
Track Labor Per Assessment
Measure completed paid assessments per provid er, labor cost per assessment, and admin hours per case. That tells you if each added person is lifting revenue enough to cover pay, support, and downtime. If a new hire adds volume but also adds coordination and payroll, owner income can stall even while top-line revenue rises.
Use a simple test: each provider should cover their own pay plus a share of admin support. Here’s the quick math to watch: revenue per assessment minus direct labor and admin cost. If that spread shrinks as headcount grows from 6 to 32, the business is scaling revenue faster than profit.
5
- Track provider utilization weekly.
- Separate owner delivery from management time.
- Price in admin and subcontractor support.
- Forecast cash for payroll timing.
Overhead And Reserves
Fixed Overhead Hurdle
Fixed overhead is the monthly floor the service has to clear before the owner can safely take money out. Here, the stated fixed cost base is $116k per month, including $45k rent, $12k liability insurance, $800 software, $30k marketing, $600 utilities, and $15k continuing education.
That means owner income depends on cash coming in faster than this load, plus enough room for reserves tied to delayed collections, device demos, credentialing, replacement tools, and slow referral months. One clean rule: if overhead is not covered first, distributions are not income, they’re stress.
Reserve Before Draw
Track a monthly reserve target as planned cash, not leftover profit. Watch collection lag, referral volume, and the size of nonbillable items that hit cash but don’t show up as revenue. If collections slow or demo costs rise, the owner’s draw should wait until the reserve is funded.
- Compare cash in to $116k overhead.
- Separate reserve money from operating cash.
- Test how delays affect monthly draw.
Tight overhead control matters most when work is steady but cash is late. If the team keeps marketing, rent, insurance, and continuing education in line, more of each collected dollar can become owner pay instead of getting absorbed by fixed costs.
6
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner income shifts fast here because revenue depends on provider count, visit volume, pricing, and capacity use. Early years run red, then earnings rise as fixed overhead gets covered.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | The low case mirrors Year 1, when the team is small and EBITDA is still negative. | The base case matches Year 3, when the model is moving past the ramp and turns profitable. | The high case mirrors Year 5, when the schedule is full and earnings are strongest. |
| Typical setup | About 6 providers, Year 1 revenue of $202k, and -$193k EBITDA leave no room for a $145k owner salary on top of operating losses. | About 18 providers, Year 3 revenue of $1.136M, and $384k EBITDA support owner pay after core overhead. | About 32 providers, Year 5 revenue of $3.036M, and $1.831M EBITDA create the best owner take-home. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$193kLaunch loss | $384kBase profit | $1.8MScale peak |
| Best fit | Use this to stress-test the launch year if referral flow or utilization runs below plan. | Use this as the main operating case for planning, hiring, and cash flow decisions. | Use this to test upside if capacity stays full and the team keeps adding volume cleanly. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. Taxes, debt, benefits, reserves, and unlisted payroll can lower take-home.
Related Products
- Assistive Technology Assessment Service Porter's Five Forces Analysis
- Assistive Technology Assessment Service BCG Matrix
- Assistive Technology Assessment Service Business Model Canvas
- What 5 KPIs For Assistive Technology Assessment Service Business?
- Assistive Technology Assessment Service Business Plan Template in Pre-Written Word
- How Increase Profitability Of Assistive Technology Assessment Service?
- What Are Operating Costs For Assistive Technology Assessment Service?
- Assistive Technology Assessment Startup Costs: $116k Monthly Overhead
- Assistive Technology Assessment Financial Model Template in Excel
- How To Open An Assistive Technology Assessment Service In 8–16 Weeks
- How To Write A Business Plan For Assistive Technology Assessment Service?
- Assistive Technology Assessment Service Marketing Mix
- Assistive Technology Assessment Service Marketing Plan
- Assistive Technology Assessment Service Business Proposal
- Assistive Technology Assessment Service PESTEL Analysis
- Assistive Technology Assessment Service Pitch Deck Example Editable PPTX
- Assistive Technology Assessment Service Business SWOT Analysis
- Assistive Technology Assessment Service Value Proposition Canvas
Frequently Asked Questions
Under the supplied assumptions, Year 1 supports about $26k before owner salary after listed direct costs and fixed overhead The model also includes a $145k CEO and Clinical Director salary, which Year 1 does not cover from operations alone By Year 2, revenue is about $5285k, so salary coverage becomes more realistic before unlisted payroll, taxes, and reserves