 Owner income$86.2k
Owner income$86.2kHow Much Do Behavioral Health Center Owners Make At $85k Monthly Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$86.2k  Net margin134%
Net margin134% Revenue for target pay$85.1k
Revenue for target pay$85.1k Business difficultyHard
Business difficultyHard


Key Takeaways
- Collections, not billed revenue, fund owner draws.
- Monthly visits above 505 cover fixed overhead.
- Payroll is the biggest margin lever.
- Payer mix and denials can cut cash.
Owner income$86.2kNet margin134%Revenue for target pay$85.1kBusiness difficultyHardWant to test your behavioral health center owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on collections, staffing, payer mix, overhead, reserves, and debt.
How does owner income show up in the Behavioral Health Center model?
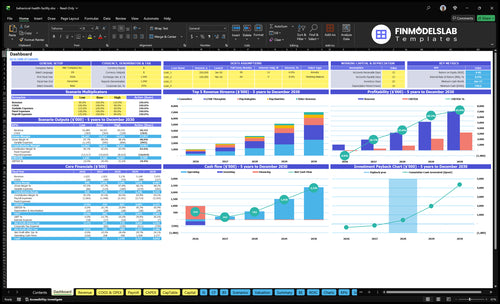
This Behavioral Health Center Financial Model Template ties payer mix, staffing, overhead, and owner income together; open it to see monthly collected revenue, EBITDA margin, break-even visits, payroll load, fixed overhead, and reserve impact.
Owner-income model highlights
- Monthly take-home view
- Revenue and margin
- 5% reserve impact
Does outpatient or residential care create higher owner income?
For a Behavioral Health Center, outpatient is not automatically better, and residential is not automatically better either. Outpatient therapy has lower facility burden, but owner income still depends on visit volume and provider utilization; this model is visit-based at 592 first-year treatment visits/month, with no bed census assumption. Intensive outpatient, partial hospitalization, residential care, and substance abuse treatment can raise revenue per client, but they also bring higher staffing, licensing, documentation, authorization, and risk costs. Income follows utilization, payer approval, and collections.
Outpatient side
- Lower facility burden
- Depends on visit count
- Needs strong provider use
- Collections drive owner pay
Residential side
- Higher revenue per client
- Higher staffing load too
- More authorization work
- More compliance risk
What profit margin can a behavioral health center expect?
A Behavioral Health Center should judge profit by operating margin, not gross revenue. The first-year model shows an EBITDA (earnings before interest, taxes, depreciation, and amortization) margin of 134% on $102 million revenue, using 90% direct plus variable costs, $212,400 fixed overhead, and $580,000 named payroll. For a How Much Does It Cost To Open A Behavioral Health Center?, a few missed visits per clinician can erase the owner draw.
Margin Drivers
- Reimbursement rates set the margin.
- Clinician productivity drives visit volume.
- 134% is the modeled EBITDA margin.
- $102 million revenue is the base case.
What Compresses It
- Benefits and supervision raise cost.
- Billing denials hit cash fast.
- Rent, malpractice, and compliance add pressure.
- Missing wage lines compress margin.
How much can a behavioral health center owner make?
A Behavioral Health Center owner can model about $86,245 in first-year take-home distributions after a 5% reserve, separate from any paid clinical wage. Track EBITDA and utilization first; What Is The Most Critical Metric To Measure The Success Of Your Behavioral Health Center? matters because this model shows $137,329 EBITDA on $102 million in annual revenue before taxes, debt service, and unprovided payroll lines.
Owner take-home
- $86,245 modeled first-year distribution
- 5% reserve held back
- $137,329 modeled EBITDA
- Clinical wage is separate income
What changes it
- Facility size and capacity
- Service mix and acuity
- Payer contracts and rates
- Utilization, payroll, compliance
Want the six income drivers that matter most?
1
$14.4K/visitPayer Mix
Better reimbursement lifts collected revenue per visit, so owner take-home improves before volume even changes.
2
592/moCensus
More filled visits spread rent and admin cost across more revenue, while empty slots cut EBITDA fast.
3
$75-$280Service Mix
More psychiatry and psychology raises revenue per slot, while groups and counseling add lower-priced volume.
4
60%-90%Staffing Productivity
Moving clinician capacity from 60% to 90% helps cover the $580K payroll base and lifts margin.
5
30 moCollections
Clean claims and prior auth turn billed visits into cash faster, which shortens payback and protects cash flow.
6
$17.7K/moOverhead
At $17,700 a month in fixed overhead, plus a 90% direct and variable cost load, small overspend hits profit hard.
Behavioral Health Center Core Six Income Drivers
Payer Mix And Reimbursement
Payer Mix And Reimbursement
Payer mix is the split of commercial insurance, Medicaid, Medicare, and cash pay, plus the allowed amount each payer contract pays. In this model, Year 1 prices run from $75 for group sessions to $250 for psychiatrist visits, but the owner only keeps what is actually collected after denials and payment lag.
Collected revenue matters more than billed revenue. The model shows $85,140 in first-year monthly collected revenue before taxes and debt, so a lower collection rate or slower payer lag cuts owner take-home before rent or payroll changes. Stronger collections lift EBITDA, or operating profit before financing and noncash charges, and build reserves.
Track cash by payer, not just visits
Measure allowed amount, collection rate, denial rate, payer lag, and revenue per visit by payer and service. That shows which visits fund owner pay and which ones sit in accounts receivable. If a payer pays less or later on a $250 visit, the same schedule produces less cash.
Use a simple weekly review: cash collected, claims denied, and days to pay. Here’s the quick math: higher net collections improve cash without adding rent or staff cost, while weak collections leave the business busy but short on cash for distributions.
- Compare cash by payer monthly.
- Flag denials within seven days.
- Track lag by service type.
1
Census, Client Volume, And Utilization
Client Volume And Utilization
Utilization means turning staffed capacity into billable visits. The model uses first-year utilization of 600% for psychiatrists, 650% for psychologists, 700% for LCSW therapists, 700% for counselors, and 600% for group facilitators, which supports about 592 treatment visits/month. That is above the 505-visit/month break-even, so each steady added visit lifts owner income without pushing fixed costs up as fast.
The risk is not demand alone. No-shows, discharge gaps, access limits, and unsustainable caseloads can pull visits below plan. If completed visits slip, cash drops before rent and admin costs change, which cuts the owner’s draw fast. Steady scheduling is the fastest way to protect profit here.
Hold The Calendar Above Break-Even
Track scheduled visits, completed visits, no-show rate, open slots, and discharge timing each week. The useful test is simple: stay above 505 visits/month and watch whether the clinic can keep filling canceled slots the same day. If completed volume falls, owner pay falls right away.
Use tight reminders, fast rebooking, and discharge follow-up to keep the 592-visit/month run rate. Watch utilization by role, not just at the clinic level, so one understaffed provider does not create a bottleneck. Full calendars fund the owner draw; empty chairs do not.
2
Service Mix And Level Of Care
Service Mix and Level of Care
Service mix changes both revenue per visit and how much labor each dollar needs. In Year 1, prices range from $75 for group sessions to $250 for psychiatrist visits, with $180 psychologist visits, $150 LCSW therapy, and $120 counselor visits. More psychiatry lifts revenue, but it also depends on scarce clinical time.
Higher-acuity care like intensive outpatient, partial hospitalization, residential care, and substance abuse programs can raise gross revenue, but they also add staffing, licensing, documentation, authorization, and compliance load. If the mix shifts up without enough clinical capacity, cash flow can slip and the owner’s draw falls even when billed revenue looks stronger.
Manage mix by margin and capacity
Track visits by service line, net collection rate, clinician hours per visit, and denial rate. The key inputs are service volume, payer payment, and staff time. A $250 psychiatry visit is not better than a $75 group session if it blocks a high-demand clinician or triggers more admin work.
Use group care to add capacity, then reserve higher-acuity programs for cases where the staff, authorizations, and documentation process can support them. The best mix is the one that raises cash after labor, not just scheduled revenue. If the service line adds compliance overhead faster than revenue, it hurts owner income.
3
Staffing Model And Clinician Productivity
Staffing and Clinician Productivity
Payroll is the biggest controllable margin lever here: Year 1 payroll is $580,000, including a $250,000 Clinical Director Psychiatrist, a $150,000 Lead Psychologist, and 2 LCSW therapists at $90,000 each. Estimate it from headcount, scheduled hours, billable visits per FTE, and loaded labor cost. If collected revenue runs $85,140/month, payroll alone is about 57% of annual collections.
That’s why full calendars fund the owner draw. When utilization rate slips, payroll stays fixed and profit gets squeezed before rent or admin do. Watch supervision load, turnover, recruiting, benefits, and admin support, because each one changes how many visits each clinician can bill. Quality, documentation, and sustainable caseloads still come first.
Track Visits per FTE
Measure each clinician’s billable visits per FTE, not just hours worked. Break out benefits, turnover, recruiting time, and admin support so you can see true labor cost per visit. If a role is paid well but stays underfilled, it drags cash flow and delays owner pay.
Use a weekly dashboard for open slots, no-show rate, and supervision hours. If productivity drops, tighten scheduling, reduce gaps between intake and follow-up, and protect documentation time so claims stay clean. Don’t push caseloads past what clinicians can sustain.
4
Billing, Collections, And Authorization Performance
Billing, Collections, and Authorization
This driver is about how much of billed care turns into cash. The model shows $85,140 in first-year monthly collected revenue before taxes and debt, so owner pay depends more on net collection rate than on scheduled visits. If claims are delayed or denied, the center can be full and still short on cash.
Watch clean claim rate, denial rate, prior authorization timing, documentation completeness, and collection lag. A visit only helps income when the claim gets paid. Medical necessity gaps and slow follow-up can cut cash even when demand is strong, which pushes out reserves and owner distributions.
Shorten the cas h cycle
Start at intake: verify eligibility, get prior auth, and complete documentation before the first visit. Then work denials daily and resubmit fast. Here’s the quick math: collected revenue equals billed revenue times the net collection rate, so even good volume misses cash if follow-up is slow.
Use a weekly dashboard for clean claim rate, denial reasons, days to collect, and unpaid authorizations. If notes are weak, fix the template and staff workflow first. Cleaner claims protect cash, reduce admin waste, and make owner draws more predictable.
5
Fixed Overhead And Compliance Costs
Fixed Overhead And Compliance Costs
Fixed overhead is $17,700 per month before clinical labor, so it hits take-home even when visit volume rises. The load includes $10,000 rent, $1,500 utilities, $800 facility insurance, $700 maintenance, $2,000 electronic health record licensing, $1,200 operational platform licensing, $500 administrative software, and $1,000 professional services.
What matters is whether monthly collected revenue clears that base after payroll and other variable costs. Below break-even, every extra month of low volume makes owner pay thinner; at higher volume, the same overhead gets spread across more visits and hurts less. Compliance creep from accreditation, audits, HR, malpractice, and marketing can quietly push this number up.
Track The Burn Before It Spreads
Keep fixed costs separate from clinical labor, reserves, and one-off projects. Track the monthly run rate for rent, software, insurance, and professional services, then test each line against visit volume and collected cash. The key question is simple: does the center clear $17,700 fast enough to leave room for owner draw?
- Watch monthly fixed cost per visit.
- Cap software and service creep.
- Review compliance spend each quarter.
If overhead rises faster than census, profit compresses even when the schedule looks full. That is why the owner should forecast fixed costs first, then build staffing and pricing around the cash left after that base is covered.
6
Compare owner income scenarios using the provided operating assumptions
Owner income scenarios
Owner income changes fast with visit volume, therapist capacity, and fixed overhead. This model moves from near break-even early on to stronger earnings as utilization fills out.
| Scenario | Low CaseThin margin | Base CaseFundable base | High CaseScale with caution |
|---|---|---|---|
| Launch model | This is the near break-even case with limited owner income. | This is the modeled operating case with modest owner income. | This is the stronger earnings path if volume and capacity keep rising. |
| Typical setup | The model sits around 505 treatment visits a month and about $72,564 in monthly revenue, with EBITDA near zero before reserves and heavy fixed overhead. | The model runs at 592 visits a month, about $85,140 in monthly revenue, and $137,329 in annual EBITDA, or about $86,245 after a 5% reserve. | Year 2 modeled revenue reaches $160,144 a month, with $875,977 in EBITDA before unprovided payroll lines and $779,891 after a 5% reserve. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0Near break-even | $86,245Modeled base | $779,891Upside case |
| Best fit | Use this to stress-test the first operating year if volume ramps slowly or staffing runs ahead of demand. | Use this as the most balanced case for planning cash, staffing, and owner draws. | Use this to test upside if referrals stay strong and staffing keeps pace with demand. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Behavioral Health Center Porter's Five Forces Analysis
- Behavioral Health Center BCG Matrix
- Behavioral Health Center Business Model Canvas
- 7 Critical KPIs to Scale Your Behavioral Health Center
- Behavioral Health Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Behavioral Health Center Profitability
- How Much Does It Cost To Run A Behavioral Health Center Monthly?
- Behavioral Health Center Startup Costs With $177K Monthly Fixed Costs
- Behavioral Health Center Financial Model Template in Excel
- How To Open A Behavioral Health Center: 6–12+ Month Launch Roadmap
- How to Write a Behavioral Health Center Business Plan
- Behavioral Health Center Marketing Mix
- Behavioral Health Center Marketing Plan
- Behavioral Health Center Business Proposal
- Behavioral Health Center PESTEL Analysis
- Behavioral Health Center Pitch Deck Example Editable PPTX
- Behavioral Health Center Business SWOT Analysis
- Behavioral Health Center Value Proposition Canvas
Frequently Asked Questions
The first-year model shows about $86,245 in potential pre-tax owner distributions after a 5% reserve That comes from $102 million in annual revenue and $137,329 in EBITDA If the owner also works as a paid clinician, that compensation is separate from profit and should not be mixed with draws