 Time to Open8-12 weeksLaunch runway
Time to Open8-12 weeksLaunch runwayHow To Open A Bereavement Counseling Service In 6 To 12 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8-12 weeksLaunch runway  Launch Sequence5 stagesCompliance first
Launch Sequence5 stagesCompliance first Key BottleneckCredentialingApproval path
Key BottleneckCredentialingApproval path First Revenue StepPaid intakeIntake ready
First Revenue StepPaid intakeIntake ready
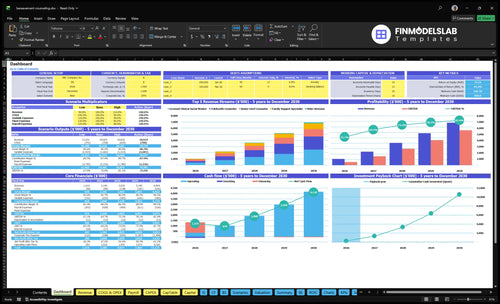


A licensed clinician can often open a lean private-pay bereavement counseling service in about 6 to 12 weeks if licensure, the Health Insurance Portability and Accountability Act (HIPAA) workflows, intake forms, telehealth or office setup, malpractice coverage, and referral outreach are ready Insurance-based revenue can take longer because payer credentialing may lag the operational opening The researched planning assumptions show Year 1 capacity across 9 service roles, with modeled monthly revenue of about $84,130 at stated utilization First revenue usually comes from converting a hospice, physician, directory, or online inquiry into a paid intake session priced in the model from $130 to $200 for most individual services
Time to Open8-12 weeksLaunch runwayLaunch Sequence5 stagesCompliance firstKey BottleneckCredentialingApproval pathFirst Revenue StepPaid intakeIntake readyLaunch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Licensing / compliance
- Scope review
- Board checks
- Insurance binder
- Compliance packet
Clinical service design
- Intake scripts
- Privacy notice
- Documentation templates
- Crisis workflow
Office / telehealth
- Lease review
- Soundproof plan
- Video setup
- Phone routing
EHR / intake
- System select
- Intake forms
- Scheduling setup
- Billing setup
Referral outreach
- Target list
- Hospice outreach
- Provider outreach
- Directory profiles
Marketing / launch
- Website copy
- Launch materials
- Intro campaign
- First sessions
Want to pressure-test launch assumptions before you start?
Open the Bereavement Counseling Service Financial Model Template to test launch timing, capacity, payer mix, runway, and breakeven at $84,130 Year 1 revenue.
Model highlights
- 9-person Year 1 team
- 19% revenue-related costs
- First operating month gap
- Tabs: services to COGS
How do you get clients for a bereavement counseling service?
First clients for a Bereavement Counseling Service usually come from trusted referral paths, not broad ads alone, so build around hospices, funeral homes, primary care providers, faith communities, employee assistance programs, and local mental health directories. If you’re mapping the launch, How To Write A Business Plan For Bereavement Counseling Service? should tie marketing to a simple path from inquiry to consultation to paid intake. Year 1 can assume 10% of revenue goes to digital marketing and referral fees, and the first revenue win is a booked intake at $150 for a Licensed Clinical Social Worker or $175 for a Senior Grief Counselor.
Trusted referral paths
- Use hospices first
- Ask funeral homes for referrals
- Reach primary care providers
- Join faith community networks
Convert leads fast
- Screen urgency and crisis risk
- Check telehealth eligibility
- Confirm payer type and location
- Move inquiry to paid intake
Do you need a license to open a bereavement counseling service?
Yes, a Bereavement Counseling Service generally needs state-recognized mental health licensure before offering grief therapy; coaching, peer support, or education can’t be sold as therapy outside legal scope. Before pricing sessions or reviewing What Are Operating Costs For Bereavement Counseling Service?, clear the first launch gate: state board rules, supervision, telehealth, advertising, documentation, and malpractice coverage.
License Gate
- Check state board rules first
- Use licensed clinical roles only
- Confirm telehealth scope by state
- Do not book therapy early
Allowed Scope
- Licensed clinical social worker
- Licensed professional counselor
- Licensed psychologist
- Other state-recognized license
What are common mistakes opening a bereavement counseling service?
For a Bereavement Counseling Service, the biggest launch mistakes are opening before compliance and crisis systems are ready, treating peer support like therapy, and assuming referrals will show up without outreach. Year 1 utilization is modeled at just 40% to 65% by role, so don’t staff or lease as if every slot fills on day one.
Fix compliance first
- Confirm state scope before opening
- Set HIPAA-ready documentation
- Build crisis escalation steps
- Separate peer support from therapy
Fix demand and intake
- Define client populations clearly
- Build referral relationships early
- Use a calm intake workflow
- Don’t assume full utilization
Confirm what must be complete before accepting grief counseling clients
Launch readiness checklist
Use this go-live approval checklist before opening the bereavement counseling practice.
Licensure
- State licensure confirmedCritical
No launch until the state license, scope, and ownership are clear for each clinician.
- Supervision authority confirmedCritical
Needed if any role works under supervision or limited scope.
- Advertising rules reviewedHigh
Keeps marketing claims, specialties, and testimonials inside state rules.
- Business registration filedCritical
The practice needs a legal entity and tax setup before contracts and payments.
Clinical
- Crisis protocol writtenCritical
Grief work can surface risk, so staff need a clear escalation path.
- Consent packet finalizedCritical
Bundle privacy, cancellation, emergency contact, and referral forms before first session.
- Emergency contacts capturedHigh
Helps reach support fast if a client becomes unsafe or unreachable.
- Documentation standards setHigh
Consistent notes protect care quality, billing, and liability.
Systems
- HIPAA EHR liveCritical
The record system must be ready for secure charting and access control.
- Billing workflow testedHigh
Test claims, payments, and denials before the first bill goes out.
- Secure video workflow testedHigh
Telehealth needs a private, stable flow before remote sessions start.
Setup
- Office or virtual setup readyHigh
Rooms, devices, internet, and privacy need to work for real sessions.
- Scheduling and phone scripts readyHigh
A clear intake script cuts missed details and speeds first bookings.
- Inquiry tracking activeHigh
Track every lead so no referral or website inquiry gets lost.
Staffing
- Roles assignedCritical
Every clinical and admin task needs one owner on day one.
- Training completedHigh
Staff should know intake, crisis steps, and tool use before opening.
- Utilization targets setMedium
Year 1 load should reflect 40% to 65% use by role.
Revenue
- Referral partners confirmedCritical
Confirmed partners create the first client flow and reduce early vacancy.
- Website is liveCritical
Prospects need a live site to learn, inquire, and book.
- Initial consult booking liveCritical
The first revenue step should route visitors straight into intake.
- Cash runway reviewedCritical
Early fixed costs are at least $9,500 per month, so cash must cover the ramp.
Want to see what drives launch readiness?
1Clinical Scope
License gateWritten board clearance keeps therapy, supervision, and telehealth legal, so launch starts without shutdown risk.
2HIPAA Protocols
Day 1 readyA complete intake, privacy, and crisis workflow cuts day-one misses and protects high-acuity clients.
3Service Positioning
Clear offerClear offers by client type and format cut confusion and lift referral conversion.
4Practice Systems
Flow testedA tested path from inquiry to note and payment keeps clients from dropping off before the first visit.
5Referral Network
Lead flowActive outreach to referral partners shortens the wait for first clients after opening.
6Payer Ramp
$84.1K/moYear 1 revenue can reach about $84.1K a month at 40%-65% utilization, but $11.9K fixed costs and credentialing can delay cash.
Clinical Licensing and Scope
License and Scope Gate
If the practice cannot prove its clinical authority first, it cannot legally open for therapy. This gate controls whether you can deliver grief counseling, supervise staff, document care, advertise services, and serve telehealth clients across state lines. One wrong assumption here can turn opening day into rework, delayed intake, or a forced pause.
The readiness signal is written confirmation of state board rules, license status, scope of practice, supervision limits, and advertising rules. Before launch, finish the board review, bind malpractice coverage at $1,200 per month, lock the supervision plan, check telehealth rules, and review every service description so the public offer matches legal authority.
Verify Authority Before Marketing
Start with a state-by-state rules matrix and keep it written. If telehealth is part of day one, confirm where the provider may treat, document, and advertise, then align the website and intake forms to that boundary. That keeps the launch clean and avoids selling a service the practice is not yet allowed to deliver.
Do the legal checks before ads, referral outreach, and scheduling. Board review first, insurance second, supervision plan third, then telehealth and ad copy. If the offer changes after clients are already in the funnel, you risk rework, delayed cash start, and a launch that looks open but still cannot accept cases.
- Confirm license scope in writing.
- Bind malpractice before intake.
- Check telehealth state rules.
- Approve supervision before hiring.
- Review every service and ad line.
1
HIPAA, Intake, and Crisis Protocols
HIPAA, Intake, and Crisis Protocols
At launch, this is the difference between a clean first week and a scramble. A counseling practice can’t safely open day one without a working intake packet that covers informed consent, privacy notice, emergency contact, payment policy, cancellation terms, release forms, documentation standards, and crisis escalation steps.
The setup also needs EHR and secure messaging, plus chart templates and a referral escalation list. Here’s the quick math: $800 per month for EHR and billing software, plus $1,200 per month for professional liability insurance, for $2,000 per month before other overhead. If high-acuity clients are accepted without emergency steps, launch risk jumps fast.
Build the intake and crisis flow before first booking
Set the paperwork and response path before taking appointments. The founder should verify the intake packet is complete, the EHR is live, secure messaging works, and every therapist knows when to escalate a crisis. No intake packet, no safe launch.
- Confirm informed consent and privacy notice
- Collect emergency contacts and release forms
- Test chart templates and note standards
- Map crisis steps and referral backups
- Bind liability coverage before opening
What this protects: fewer missed steps, cleaner records, and safer first-day care. What it hides: if any step is manual or unclear, staff will slow down, clients may wait longer, and the practice can feel unready even if the calendar is full.
2
Bereavement Service Positioning
Clear Grief Service Menu
Bereavement counseling can’t launch with a generic “we help with grief” message. The readiness signal is a defined offer: who it serves, whether it is individual, family, group, or telehealth, how acute the case can be, and who pays. That clarity is what lets referral partners send the right clients on day one.
Year 1 pricing needs to match the offer mix: $175 Senior Grief Counselor, $150 Licensed Clinical Social Worker, $200 Family Support Specialist, $60 group session, and $130 Telehealth Counselor. If those prices and use cases are not tied to a clean menu, you get mismatched leads, slower intake, and weaker first-month cash.
Lock the Offer Before Opening
Before launch, write the service map in plain English: client type, session format, acuity boundary, payer path, and telehealth availability. Then turn that into one-page service sheets, referral scripts, and website copy so people know exactly which option fits each case. No clear positioning means slow intake.
- Define each service by client fit.
- Match each session type to a price.
- Set telehealth rules before marketing.
- Train referral partners on case boundaries.
- Flag high-acuity cases for escalation.
If any of those inputs are vague, opening may still happen, but the team will spend day one rewriting messages instead of filling the calendar. That slows conversion to intake and confuses the people sending referrals.
3
Practice Systems and Client Workflow
Practice Systems and Client Flow
For a grief counseling practice, the launch risk is not just getting inquiries. It’s making sure each person can move from inquiry to consult, intake, session, payment, note, and follow-up without friction. If that path breaks, you lose clients before the first appointment, which slows opening and hurts trust on day one.
This setup includes secure video or office flow, scheduling, phone coverage, billing, EHR templates, intake routing, and a missed-appointment process. Year 1 adds 3% EHR transaction fees, 2% clinical intake materials and assessments, and 4% telehealth platform usage fees. Calm systems matter here because the client’s first contact often happens during a hard week.
Test the Intake-to-Session Path
Before opening, run the full workflow end to end: inquiry, consult booking, intake forms, consent, payment, note, and follow-up task. Check that the handoff is fast, the instructions are clear, and staff know what happens if someone misses a call or a session. One weak step can drop the lead.
- Confirm phone and message coverage
- Load EHR note templates
- Route intake forms automatically
- Set missed-appointment rules
- Test telehealth and office steps
Here’s the quick math: if intake slips create even a small loss between inquiry and first visit, you feel it right away in a small practice. Clean systems protect first revenue, reduce rework, and keep the client experience steady when emotions are already high.
4
Referral Network and Local Demand
Referral Network Readiness
If this service opens without warm referral paths, the first weeks can be slow, even if the calendar and licenses are ready. For bereavement counseling, hospices, funeral homes, primary care providers, faith communities, employee assistance programs, and local directories are the early demand engine, so this work affects whether the practice gets its first client flow on time.
Here’s the quick math: the Year 1 model carries 10% digital marketing and referral fees, then that cost should fall as referral efficiency improves. If outreach starts after opening, the bottleneck is not clinical capacity, it’s waiting for clients. Active referrals before day one support a steadier first-client flow and a faster utilization ramp.
Build Referrals Before Opening
Set up the referral system before launch: referral one-sheet, website service page, inquiry script, provider email sequence, local search setup, and referral tracking. That is the minimum stack for outreach, follow-up, and measuring which channels actually send clients. One clean sentence matters: every referral partner should know who you help, how to contact you, and what happens next.
Verify the handoff is live before opening day. Test the intake response time, confirm the website page is searchable, and assign follow-up calls so no lead goes cold. If outreach is weak, the practice may open legally but still sit idle, which hurts cash flow, staff utilization, and the client experience in the first month.
- Contact referral partners before opening
- Track every source from day one
- Follow up within one business day
- Keep the service page simple
- Review the 10% Year 1 cost line
5
Payer Strategy and Revenue Ramp
Payer Mix and Cash Ramp
This driver decides whether the practice opens with cash coming in on day one, or only looks open while claims sit in credentialing. Private-pay starts faster than insurance-heavy models, but insurance can widen access later. The risk is confusing booked sessions with reimbursed revenue, especially when the Year 1 plan still assumes 40% to 65% utilization before the ramp is fully built.
The plan needs a clear payer mix: private-pay, insurance, employee assistance programs, groups, telehealth, or a hybrid setup. With monthly treatment assumptions of 100 Senior Grief Counselor sessions, 120 Licensed Clinical Social Worker sessions, 80 Family Support Specialist sessions, 40 group sessions, and 140 Telehealth Counselor sessions per provider, modeled monthly revenue at utilization is about $84,130.
Lock the Cash Order First
Before opening, sequence the payer work around cash timing, not best-case demand. Start with the services that can bill fastest, then add insurance only after credentialing dates, billing rules, and payer documents are set. One clean rule: open only the services you can bill correctly.
- Confirm credentialing lead times.
- Map each service to a payer.
- Test billing for every session type.
- Reserve cash for slow reimbursement.
Document which offers are private-pay on day one, which need approval, and which stay on hold. If the launch happens before reimbursement is live, payroll, EHR, billing, and insurance costs still hit the bank account right away, so the staffing plan has to fit the slowest cash month.
6
Related Products
- Bereavement Counseling Service Porter's Five Forces Analysis
- Bereavement Counseling Service BCG Matrix
- Bereavement Counseling Service Business Model Canvas
- What Are 5 KPIs For Bereavement Counseling Service Business?
- Bereavement Counseling Service Business Plan Template in Pre-Written Word
- How Increase Bereavement Counseling Service Profits?
- What Are Operating Costs For Bereavement Counseling Service?
- Bereavement Counseling Service Startup Costs: $860K Cash Plan
- Bereavement Counseling Financial Model Template in Excel
- How Much Bereavement Counseling Owners Make On $10M-$69M Revenue
- How To Write A Business Plan For Bereavement Counseling Service?
- Bereavement Counseling Service Marketing Mix
- Bereavement Counseling Service Marketing Plan
- Bereavement Counseling Service Business Proposal
- Bereavement Counseling Service PESTEL Analysis
- Bereavement Counseling Service Pitch Deck Example Editable PPTX
- Bereavement Counseling Service Business SWOT Analysis
- Bereavement Counseling Service Value Proposition Canvas
Frequently Asked Questions
Yes, if state licensure and telehealth rules allow it A telehealth-first launch can fit the 6 to 12 week lean timeline because it reduces office setup The model includes Telehealth Counselors at 140 monthly treatments each, priced at $130 in Year 1, with 55% modeled utilization