 Owner income$516k-$5.65M
Owner income$516k-$5.65MHow Much Bereavement Counseling Owners Make On $10M-$69M Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$516k-$5.65M  Net margin51%-82%
Net margin51%-82% Revenue for target pay$1.01M-$6.90M
Revenue for target pay$1.01M-$6.90M Business difficultyMedium
Business difficultyMedium


Key Takeaways
- Collected fees rise from $15,132 to $16,961 by Year 5.
- Completed sessions drive income; 6,672 grows to 40,704.
- Associate hires must replace lost owner billable time.
- Direct costs fall to 35%, but overhead still matters.
Owner income$516k-$5.65MNet margin51%-82%Revenue for target pay$1.01M-$6.90MBusiness difficultyMediumWant to test your owner take-home?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Bereavement Counseling Service model?
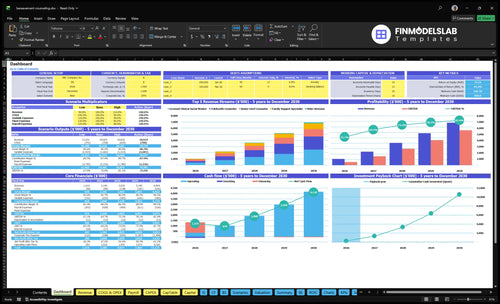
See the Bereavement Counseling Service Financial Model Template dashboard for revenue, gross profit, costs, reserves, and owner take-home—open the model.
Owner-income model highlights
- Revenue and gross profit
- Completed sessions and fee
- Direct cost percentages
- Owner take-home output
- Year 1–5 assumptions
- 9–37 clinicians modeled
- 556–3,392 sessions monthly
- $1,009,560–$6,903,840 revenue
- 50%–35% direct costs
Can a bereavement counseling owner make more by hiring clinicians?
Yes, but not automatically. In the Bereavement Counseling Service, clinician count rises from 9 in Year 1 to 37 in Year 5, monthly completed sessions grow from 556 to 3,392, and revenue climbs from $1,009,560 to $6,903,840; that only helps if utilization stays strong and overhead stays in line. Scaling can lift revenue, but it does not guarantee higher owner take-home. Groups add revenue too, but they stay a small share in the numbers provided.
Growth drivers
- 9 clinicians in Year 1
- 37 clinicians in Year 5
- 556 sessions monthly in Year 1
- 3,392 sessions monthly in Year 5
Owner take-home risks
- Ramp-up time cuts early output
- Credentialing slows clinician start dates
- Supervision adds payroll load
- Benefits and payroll taxes raise cost
How much can a bereavement counseling practice owner make per year?
A Bereavement Counseling Service owner’s yearly take-home can’t be stated from this model because it stops at revenue and gross profit, not final income after payroll, overhead, reserves, debt service, and taxes; see What Are Operating Costs For Bereavement Counseling Service? for the cost side. The supported range is $959,082 gross profit on $1,009,560 Year 1 revenue to $6,662,206 gross profit on $6,903,840 Year 5 revenue.
Owner take-home view
- Starts after clinician payroll
- Depends on owner clinical hours
- Changes with overhead control
- Excludes taxes and debt service
Model math
- Year 1 revenue: $1,009,560
- Year 1 gross profit: $959,082
- Year 5 revenue: $6,903,840
- Year 5 gross profit: $6,662,206
Is cash-pay or insurance better for a grief counseling practice owner?
For a Bereavement Counseling Service, cash-pay is usually simpler, but the real question is payer-mix sensitivity, not billing ideology; use collected fee, not list price, when you model revenue. If you want the planning version, start with How To Write A Business Plan For Bereavement Counseling Service? and test how the mix moves revenue from $151.32 in Year 1 to $169.61 in Year 5 as prices rise from $60-$200 to $80-$225. Cash-pay cuts billing friction, but insurance, EAP, sliding scale, and out-of-network collections can add write-offs, denials, admin cost, and payment timing risk.
Cash-pay
- Fewer claims, less admin work.
- Faster cash, less payment lag.
- Less friction for self-pay clients.
- Access can shrink without coverage.
Mixed payer mix
- Insurance can widen reach.
- EAP can fill unused capacity.
- Sliding scale lowers collected fee.
- Out-of-network raises write-off risk.
Which drivers move owner income most?
1
$15.1K-$17.0KAverage Fee
Higher collected fees raise revenue without adding visits, so more of each session can reach owner take-home.
2
556-3,392/moSession Volume
More completed sessions drive the top line fast, and the model scales from 556 monthly sessions to 3,392.
3
9-37Clinician Leverage
Adding associate clinicians expands billable hours faster than fixed costs, which is where profit starts to widen.
4
1.0 FTEOwner Capacity
Protecting the owner's clinical time from admin work keeps paid sessions high and supports stronger personal income.
5
$11.5K-$122.9KGroup Mix
Group and workshop revenue adds lower-cost income, so a bigger mix can lift cash profit with less staff time.
6
50%-35%Cost Discipline
Keeping direct costs and reserves tight matters because every point of margin protection flows straight to owner cash.
Bereavement Counseling Service Core Six Income Drivers
Average Collected Fee And Payer Mix
Collected Fee and Payer Mix
Owner income rises when each completed session brings in more collected cash, not just a higher list price. In this model, average collected fee moves from $15132 in Year 1 to $16961 in Year 5, while posted prices range from $60 group sessions to $200 family support, then $80 to $225. The risk is simple: strong demand does not pay the bills if discounts, denials, or write-offs eat the cash.
Track Net Cash per Session
Measure net collected fee per completed session each month. Break it into list price, sliding-scale discounts, claim denials, write-offs, and payment processing fees. If the cash collected per session slips, owner pay falls even when the schedule looks full. The clean test is whether payer mix and pricing raise net cash without hurting access or completion rates.
- Track cash by service type.
- Separate billed and collected amounts.
- Watch denials and write-offs.
- Review discounts by client segment.
1
Completed Billable Session Volume
Completed Billable Sessions
Completed billable sessions are the revenue event here, not inquiries or booked visits. At 556 monthly completed sessions in Year 1 and 3,392 in Year 5, volume rises about 6.1x, from 6,672 to 40,704 sessions a year. More completed sessions spread fixed costs over more cash-producing visits, which is what protects owner pay.
The model only works if scheduled demand turns into real visits. The disclosed capacity assumption moves from 400%-650% in Year 1 to 800%-850% in Year 5, so cancellations, no-shows, seasonality, retention, and referral quality decide whether the calendar becomes revenue. One missed session is lost income, and it hits margin fast.
Protect Session Completion
Track the completion rate (completed sessions ÷ scheduled sessions), plus no-show rate and rebook rate by clinician and referral source. That shows which leads become cash and which ones just fill the calendar. If a referral source books well but completes poorly, it is noise, not growth.
- Completed sessions by month
- No-shows and late cancels
- Rebook rate after first visit
- Referral source completion rate
- Seasonality by month
Use waitlists, reminder texts, and fast rebooking after missed visits to keep completed volume stable. If demand spikes in one month and fades in the next, forecast owner draws on the lower month so cash does not get overcommitted. More completed sessions only help income when they actually show up and stay on schedule.
2
Owner Clinical Hours And Admin Load
Owner Clinical Hours And Admin Load
Owner take-home depends on whether the owner is paid for client sessions, management work, or both. Admin work here includes intake calls, billing review, supervision, referral outreach, scheduling, and compliance. If the owner gives up billable time to run the practice, that lost session revenue has to be replaced by staff margin or profit drops.
The model does not state owner clinical hours, so keep owner compensation separate from business profit. At the modeled scale, monthly completed sessions rise from 556 in Year 1 to 3,392 in Year 5, so admin load can easily turn into a real labor cost instead of “free” owner time.
Track Billable Time Versus Admin Time
Measure billable hours, admin hours, and associate contribution margin each week. Use completed sessions, not booked visits, because cancellations and no-shows still consume time. If the owner is managing growth, staff revenue must cover the owner’s lost sessions plus the extra supervision and scheduling load.
- Owner clinical hours
- Admin hours by task
- Collected fee per session
- Net margin per associate hour
One simple test: lost owner session revenue must be offset by net clinician margin. If admin starts crowding out client work, cut low-value tasks, tighten billing flow, or add staff only when their margin clearly replaces the owner’s billable hours.
3
Associate Clinician Leverage
Associate Clinician Leverage
Owner income rises when the calendar is no longer capped by one clinician. Here, staffing grows from 2 to 6 senior grief counselors, 3 to 12 licensed clinical social workers, 1 to 5 family support specialists, 1 to 4 group facilitators, and 2 to 10 telehealth counselors, so revenue can scale beyond owner hours.
But the gain only shows up after each hire covers payroll split, benefits, payroll taxes, credentialing delays, supervision, and referral demand. The quick test is simple: if a clinician’s collected revenue during ramp-up does not exceed fully loaded cost, owner take-home drops before it improves. One empty chair is expensive.
Track Ramp and Utilization
Build the forecast around collected revenue per clinician, not headcount. Track scheduled sessions, completed sessions, utilization, payer mix, and days from hire to first paid visit. If a role is slow to fill, model the lost margin from idle capacity and the owner’s missed billable hours.
Use a simple monthly check: sessions collected minus fully loaded clinician cost. That full cost should include salary or split, benefits, payroll taxes, supervision time, and admin time tied to onboarding. If referral demand cannot support the added staff, pause hiring before fixed payroll drags down cash flow.
4
Groups, Workshops, And Service Mix
Group Sessions
Group work can raise revenue per clinician hour when it fits the client’s needs and stays within licensing rules. Here’s the quick math: group therapy facilitator revenue rises from $11,520 in Year 1 to $122,880 in Year 5 as monthly completed group sessions increase from 16 to 128 and price moves from $60 to $80. Groups add cash, but they do not replace individual care in the model.
Track Fill Rate
Measure completed sessions, not just scheduled slots. The key inputs are demand, attendance, facilitator time, and room or telehealth capacity. If attendance slips, revenue drops fast because one canceled seat cuts group income with no extra labor sold. Use a simple weekly check: sessions planned, sessions filled, and cash collected. That tells you whether the group mix is really improving owner pay.
5
Overhead, Billing, Marketing, And Reserves
Overhead, Billing, Marketing, and Reserves
Owner pay rises when revenue outpaces fixed overhead and cash set aside for reserves. Here, listed direct costs are 50% in Year 1 and 35% in Year 5, driven by electronic health record transaction fees at 30% then 25%, plus clinical intake materials at 20% then 10%. That 15-point drop helps, but it does not pay the owner by itself.
Still model rent, billing, marketing, insurance, admin help, reinvestment, debt service, and reserves before any distribution. The key inputs are collected revenue, direct-cost rate, and monthly fixed costs. If those cash costs rise faster than sessions, take-home shrinks even when top-line revenue grows.
Track cash costs before owner draw
Measure collected revenue versus all-in overhead each month, not just scheduled sessions. Split costs into variable direct costs and fixed overhead, then reserve cash for slow months, denied claims, and delayed payments. In this model, the direct-cost load falls from 50% to 35%, so the next control point is overhead discipline.
One clean rule: if fixed costs and reserves take too much of each dollar, owner income lags. Watch billing cycle time, marketing spend, and admin hours; cut anything that does not lift completed sessions or collections. Keep debt service and reserves in the forecast before setting a draw.
6
Compare low, base, and high bereavement counseling income scenarios
Owner income scenarios
Session volume, clinician mix, and pricing move owner income fast here, while payroll and overhead absorb a big share. These three cases show the gap between a slow start, the model path, and upside.
| Scenario | Low CaseDownside case | Base CaseModel case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower-income path if client load and utilization lag. | This is the modeled middle path at the Year 3 operating level. | This is the stronger earnings path if hiring and sessions scale to plan. |
| Typical setup | Nine clinicians, 556 monthly completed sessions, a $15,132 average collected fee, about $1,009,560 revenue, and roughly 95% gross margin before payroll and overhead. | Twenty-two clinicians, 1,900 monthly completed sessions, a $15,922 average collected fee, about $3,630,240 revenue, and roughly 96.2% gross margin before payroll and overhead. | Thirty-seven clinicians, 3,392 monthly completed sessions, a $16,961 average collected fee, about $6,903,840 revenue, and roughly 96.5% gross margin before payroll and overhead. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $959,082Year 1 floor | $3,492,291Year 3 center | $6,662,206Year 5 upside |
| Best fit | Use this to stress-test a slower intake ramp and higher referral spend. | Use this for planning around the Year 3 operating target and steady utilization. | Use this if you expect fast hiring, fuller schedules, and stronger telehealth use. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Bereavement Counseling Service Porter's Five Forces Analysis
- Bereavement Counseling Service BCG Matrix
- Bereavement Counseling Service Business Model Canvas
- What Are 5 KPIs For Bereavement Counseling Service Business?
- Bereavement Counseling Service Business Plan Template in Pre-Written Word
- How Increase Bereavement Counseling Service Profits?
- What Are Operating Costs For Bereavement Counseling Service?
- Bereavement Counseling Service Startup Costs: $860K Cash Plan
- Bereavement Counseling Financial Model Template in Excel
- How To Open A Bereavement Counseling Service In 6 To 12 Weeks
- How To Write A Business Plan For Bereavement Counseling Service?
- Bereavement Counseling Service Marketing Mix
- Bereavement Counseling Service Marketing Plan
- Bereavement Counseling Service Business Proposal
- Bereavement Counseling Service PESTEL Analysis
- Bereavement Counseling Service Pitch Deck Example Editable PPTX
- Bereavement Counseling Service Business SWOT Analysis
- Bereavement Counseling Service Value Proposition Canvas
Frequently Asked Questions
The provided model shows $1,009,560 in Year 1 revenue and $6,903,840 in Year 5 revenue That growth comes from clinician count rising from 9 to 37 and monthly completed sessions rising from 556 to 3,392 Revenue is not owner income because payroll, overhead, reserves, and taxes still come out