 Time to Open6 monthsSetup window
Time to Open6 monthsSetup windowHow to Open a Chronic Pain Management Clinic in 4 to 9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckCredentialing gatePayer approvals
Key BottleneckCredentialing gatePayer approvals First Revenue StepCompleted visitsReferral intake
First Revenue StepCompleted visitsReferral intake


You’re opening a medical clinic where compliance, staffing, payer approval, and referrals all have to line up before the first patient visit This launch guide covers the practical sequence to start a chronic pain clinic in the United States, using a 4 to 9 month planning window and a 5-year operating model for validation
Time to Open6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckCredentialing gatePayer approvalsFirst Revenue StepCompleted visitsReferral intakeLaunch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11
Legal / compliance
- License review
- Controlled protocol draft
- Policy pack
- Compliance signoff
Facility / equipment
- Build-out scope
- Renovation work
- Equipment install
- Room setup
Payer enrollment
- Payer list
- Enrollment packets
- Submit applications
- Claim testing
Clinical staffing
- Recruit clinicians
- Offer contracts
- Onboard team
- Coverage schedule
EHR / workflows
- EHR build
- Billing setup
- Template testing
- Staff training
Referral marketing
- Referral outreach
- Patient materials
- Soft launch
- Go-live review
Why test launch assumptions before opening a Chronic Pain Management Clinic?
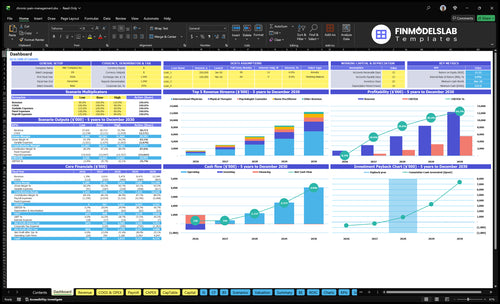
This screenshot and Chronic Pain Management Clinic Financial Model Template show revenue, costs, assumptions, cash, and break-even; open it.
Launch model highlights
- 1 physician, 2 PTs
- $116.3k monthly revenue
- $23.1k fixed overhead
- 145% Year 1 costs
- Payer timing shifts runway
How long does payer credentialing take for a pain clinic?
For a Chronic Pain Management Clinic, payer credentialing often helps set the opening date, and it sits inside the broader 4 to 9 month launch window. Do not wait until buildout is done; credentialing, provider enrollment, billing setup, and EHR configuration can all move the date. If approvals lag, cash flow lags too, because insured visits may not be billable in-network. Readiness means the applications, payer portal access, eligibility checks, coding workflow, claim submission testing, and denial follow-up are all complete.
What must be ready
- Applications filed and tracked
- Portal access confirmed
- Eligibility checks working
- Fee schedules loaded
What delays cash flow
- Provider enrollment still pending
- Tax details or bank setup missing
- Claim testing not completed
- Denial follow-up not in place
How does a pain management clinic get first patients?
A Chronic Pain Management Clinic gets first patients by converting compliant referrals and payer-approved patients into completed appointments. For startup context, see How Much Does It Cost To Open And Launch Your Chronic Pain Management Clinic?; the early win is fast scheduling, insurance verification, and referral follow-up that gets the visit kept. With more than 51 million U.S. adults living with chronic pain, the first pipeline should come from local referral partners, not fee-for-referral deals.
Referral sources
- Primary care sends the first referrals.
- Orthopedics and neurology fit next.
- Physical therapy and behavioral health help too.
- Use workers’ compensation contacts where appropriate.
Front desk system
- Set a records request workflow.
- Verify insurance before the first visit.
- Use fast scheduling callbacks.
- Track referred, scheduled, completed, billed.
Year 1 team
- Plan around 1 physician.
- Add 2 physical therapists.
- Include 1 counselor.
- Staff 1 nurse practitioner and 1 acupuncturist.
Ethical growth
- Use ethical medical marketing only.
- No fee-for-referral arrangements.
- Build payer directory listings.
- Keep referral intake scripts tight.
What mistakes cause pain clinic launch risks?
Opening a Chronic Pain Management Clinic too early usually fails for simple reasons: payer approvals aren’t in place, referral flow is weak, and intake or billing steps aren’t tested. Here’s the quick math: the model shows $116,300 in monthly revenue, but variable cost load is 145% and fixed overhead is $23,100 before wages, so a bad launch can burn cash fast. With 51 million U.S. adults living with chronic pain, demand is real, but if onboarding drags, churn risk rises before the first visit.
Launch checks
- Get payer approvals first
- Verify benefits before visits
- Use referral intake queue
- Sign malpractice coverage
Risk controls
- Train staff on intake
- Use EHR templates
- Set denial management process
- Track supervision and PDMP workflow
Confirm the clinic is ready before day one
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening moves into execution.
Regulatory
- Entity formedCritical
The clinic needs a legal entity before contracts, payroll, and licensing work can move forward.
- Ownership review completeCritical
Physician ownership and control rules must be clear before opening under state medical rules.
- Licenses verifiedCritical
Every treating clinician needs current state licensure before any patient visit starts.
- DEA registration filedHigh
Controlled-substance prescribing needs DEA approval where the clinic plan includes it.
- Malpractice boundCritical
Coverage should be active before the first patient is seen to avoid launch-day exposure.
Facility
- Lease fully approvedCritical
The clinic needs a secured site before build-out spend and vendor installs begin.
- Build-out passed inspectionCritical
Rooms, flow, and patient privacy must work before the site opens to the public.
- Equipment installed and testedHigh
Pain treatment equipment must work before any scheduled procedure or therapy visit.
- OSHA safety setup completeHigh
Safety controls protect staff and patients and reduce launch delays from avoidable issues.
Systems
- EHR configuredCritical
The EHR must support charting, orders, and records before the first appointment.
- Billing workflow testedCritical
Claims and payment flow need testing so revenue does not stall after opening.
- Scheduling and phones liveHigh
Patients need a working path to book, reschedule, and reach the clinic on day one.
- Intake forms loadedHigh
Intake forms collect history and consent before the first visit, which speeds safe care.
Staffing
- Year 1 staff hiredCritical
Year 1 staffing should match the plan: 1 physician, 2 therapists, 1 counselor, 1 NP, 1 acupuncturist.
- Credentialing files completeCritical
Payer and facility credentialing should be ready before the clinic starts billing.
- Clinical training signed offHigh
Staff must know prescribing, documentation, handoffs, and escalation steps before opening.
- Coverage schedule setHigh
The clinic needs a clear coverage plan so patient flow does not break on launch week.
Referrals
- Referral script approvedHigh
A compliant referral script helps outside doctors send the right patients from day one.
- Payer credentialing completeCritical
Claims can stall fast if payer approval work is not finished before launch.
- Directory listings liveHigh
Payer directory listings help patients find the clinic and support first visits.
- Follow-up process readyHigh
Closed-loop follow-up keeps referrals from going cold and protects first-month volume.
Finance
- Overhead model reviewedCritical
Modeled revenue is near $116,300 a month, so cost control must be checked before opening.
- Cash runway confirmedCritical
Minimum cash lands at $338,000 in Month 12, so runway needs to cover the early drawdown.
- Vendor contracts signedHigh
Core vendors like EHR, IT, insurance, and cleaning must be locked before go-live.
- Launch signoff completedCritical
Final signoff should confirm compliance, staffing, systems, referrals, and cash are all ready.
Want the six pain clinic launch drivers?
1Compliance
License gateControls launch permission and cuts the risk of ownership, prescribing, or payer issues after lease sign.
2Provider Staffing
6-clinician mixDay-one coverage depends on credentialed clinicians, so capacity opens only when the staff mix is in place.
3Payer Billing
4-9 moClean payer setup speeds first cash and reduces unpaid visits during the 4-9 month launch window.
4Clinic Workflow
$23.1K baseRight-sized rooms, EHR templates, and intake flow cut day-one workarounds and keep visits moving.
5Referral Pipeline
40% revReferral outreach lifts early utilization, which matters if opening demand starts below the Year 1 capacity plan.
6Risk Controls
Audit-readyStrong charting and risk checks lower regulatory exposure and make claims cleaner from the start.
Compliance and licensing readiness
Licensing and compliance
A chronic pain clinic cannot open on time until the state medical board, provider licenses, ownership structure, malpractice coverage, HIPAA, and OSHA basics are cleared. If the clinic will prescribe controlled drugs, DEA and state registrations, plus a prescription drug monitoring program workflow, need to be in place before the first visit. Miss one gate and the lease or payer work can stall a launch.
The real risk is finding an ownership or prescribing limit after you have already signed space or filed payer applications. That can mean rework, delayed credentials, and no day-one billing. Start with counsel review, then lock the policy binder, documentation templates, and staff training so the clinic can see patients, chart cleanly, and bill without avoidable gaps.
Clear the gates early
Build the compliance checklist before hiring or scheduling. Verify each provider’s license, confirm who can own the entity, and check whether controlled-substance rules apply to the service mix. Then line up malpractice, payer enrollment, and any required federal or state registrations so the setup matches the clinic’s actual scope.
Here’s the quick order: license, ownership, insurance, payers, drug rules, then training. Use written policies, intake and consent templates, and a PDMP check step before opening the schedule. If any item is unresolved, do not treat opening day as firm.
- Confirm state medical board rules first
- Map ownership and prescribing rights
- Bind malpractice before first booking
- Train staff on HIPAA and OSHA
- Test PDMP and chart templates
1
Provider and clinical staffing readiness
Provider and clinical staffing readiness
Day-one capacity in a chronic pain clinic depends on whether every clinician is credentialed and scheduled before opening. The Year 1 model assumes 1 interventional pain physician, 2 physical therapists, 1 psychologist counselor, 1 nurse practitioner, and 1 acupuncturist; if one role is missing, the clinic can’t cover evaluation, therapy, counseling, medication management, and complementary care at launch.
This driver also depends on payer enrollment and malpractice coverage. If credential files, supervision, or visit types are late, the result is empty slots, longer waits, and a weak first month. The bottleneck is qualified pain provider availability, so hiring speed and credential review set the real opening date.
Build the staffing grid first
Map each role to a visit type before you lock the schedule. Assign room use, intake coverage, follow-up slots, and supervision rules in writing so the front desk can book without guessing. That keeps the clinic from opening with paper staffing but no real appointment supply.
Before go-live, verify credential files, payer status, and malpractice effective dates for every clinician. Then test a full week of schedules against the Year 1 mix so you can see if the team can support first-day demand across evaluation, therapy, counseling, medication management, and acupuncture.
- Confirm supervision before booking visits.
- Match rooms to service type.
- Block intake and follow-up coverage.
- Stress-test provider calendars in advance.
2
Payer credentialing and billing readiness
Payer Credentialing
For a chronic pain clinic, payer approval timing drives when cash starts. If applications, contracted rates, or insurance enrollment lag inside the 4 to 9 month launch window, the clinic may still open, but first visits can sit unpaid. Clean claims from day one depend on coding accuracy, eligibility checks, and the right billing workflow.
Here’s the quick math: Year 1 billing system fees are modeled at 25% of revenue, so setup has to be tight before the first appointment. Fee schedule setup, payer portal access, benefits verification, prior authorization if needed, coding review, denial queue handling, and payment posting all affect whether visits turn into collected revenue or denied claims.
Credentialing checklist
Start payer applications early and track each payer by status, missing document, and expected approval date. Verify contracted rates, enrollment files, and portal access before scheduling volume ramps. Also confirm who owns eligibility checks and prior authorization so front desk, billing, and clinicians do not step on each other.
Test at least one claim from a real visit flow before opening wide. That means checking coding review, claim transmission, denial handling, and payment posting in the same sequence the clinic will use on day one. If that loop fails, cash slows, unpaid visits rise, and the opening plan needs more working capital.
3
Facility and clinical workflow setup
Right-Sized Clinic Setup
The clinic has to match its actual first-year scope: physician visits, physical therapy, counseling, nurse practitioner visits, and acupuncture. If you overbuild for procedures you are not offering yet, you add delay and cash burn without helping day-one care. The listed fixed overhead already totals $23,100 per month, so every extra room, vendor, or system should earn its keep.
Opening on time depends on having the right rooms, the right forms, and the right flow. That means exam rooms, therapy space, procedure readiness only if it is actually in scope, plus supplies, pharmaceuticals policy, EHR templates, scheduling rules, intake forms, referral records, consent forms, and vendor setup. Miss any of those, and staff start using workarounds on day one.
Build the Day-One Workflow
Set up the patient path before the first appointment is booked. Here’s the quick math: if a visit needs a room, a chart, a consent form, and a booked slot, then one missing step slows the whole chain. Test room turns, chart templates, and intake flows with the exact visit types you plan to offer. That keeps the clinic from opening with manual gaps.
- Map each visit type to a room.
- Load intake and consent forms first.
- Set scheduling rules by service length.
- Confirm referral records before launch.
- Lock vendor setup before opening day.
What this setup hides is timing risk. If the EHR subscription, IT support, or cleaning vendor starts late, staff lose time on day one fixing basic tasks instead of seeing patients. The goal is simple: make the first week run on the system, not on email threads and handoffs.
4
Referral pipeline and patient acquisition
Referral Pipeline and Patient Flow
This driver decides whether the clinic opens with booked visits or empty slots. Pre-launch outreach to referring physicians, local search presence, payer directory visibility, and fast scheduling all shape day-one demand, so weak setup here can delay usable opening even if the space is ready.
The bottleneck is a thin referral base at launch. With 40% of revenue modeled for Year 1 patient acquisition, the clinic needs referral packets, records transfer, and appointment conversion tracking in place before opening, or the first weeks will rely on slow organic demand instead of planned utilization.
Pre-Open Referral Setup
Build outreach lists for 6 referral groups: primary care, orthopedics, neurology, physical therapy, behavioral health, and workers’ compensation where relevant. Send referral packets early, set response-time targets, and test records transfer before go-live so outside offices can send patients without back-and-forth.
Track each referral from first contact to scheduled visit. If directory listings are incomplete or scheduling is slow, conversion drops and day-one capacity stays underused. That also raises cash pressure, because fixed clinic costs start before referral volume catches up.
- Verify payer directory listings.
- Test referral-to-appointment flow.
- Document conversion by source.
- Assign one owner for follow-up.
5
Risk controls and documentation systems
Documentation and risk controls
The clinic can’t open cleanly if each provider documents pain plans, follow-ups, and refills in a different way. With 51 million US adults living with chronic pain, the first day has to be safe, consistent, and auditable. That means EHR templates, informed consent, referral notes, follow-up rules, and opioid-risk controls where relevant must be set before scheduling starts.
The launch risk is simple: inconsistent charts slow care, weaken claims, and raise regulatory exposure. If clinical leadership and compliance have not signed off on the policy set, staff training, PDMP checks where required, incident reporting, and chart audits, the clinic may still open the doors but won’t be ready to manage higher-risk medication visits or defend decisions in a review.
Build the charting rules first
Lock the rules before the first appointment. Use one template set for treatment plans, refill rules, escalation steps, and quality checks, then train every provider on the same workflow. If urine drug screening is used, spell out who orders it, when, and how results change the plan.
- Approve templates before onboarding.
- Test PDMP and consent workflows.
- Audit charts in week one.
That sequencing protects day-one care and keeps the team from improvising when volume picks up.
6
Related Products
- Chronic Pain Management Clinic Porter's Five Forces Analysis
- Chronic Pain Management Clinic BCG Matrix
- Chronic Pain Management Clinic Business Model Canvas
- 7 Financial and Operational KPIs for Chronic Pain Management Clinics
- Chronic Pain Management Clinic Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Chronic Pain Management Clinic Profit Margins
- How Much Does It Cost To Run A Chronic Pain Management Clinic Monthly?
- Chronic Pain Management Clinic Startup Costs: $600K+ CAPEX
- Chronic Pain Management Clinic Financial Model Template in Excel
- How Much Chronic Pain Management Clinic Owners Can Take Home: $351K–$651K
- How to Write a Chronic Pain Management Clinic Business Plan
- Chronic Pain Management Clinic Marketing Mix
- Chronic Pain Management Clinic Marketing Plan
- Chronic Pain Management Clinic Business Proposal
- Chronic Pain Management Clinic PESTEL Analysis
- Chronic Pain Management Clinic Pitch Deck Example Editable PPTX
- Chronic Pain Management Clinic Business SWOT Analysis
- Chronic Pain Management Clinic Value Proposition Canvas
Frequently Asked Questions
Start with the services you can staff, bill, document, and supervise safely on day one The base model uses 5 clinician categories in Year 1: 1 interventional physician, 2 physical therapists, 1 counselor, 1 nurse practitioner, and 1 acupuncturist Add procedure capability only when facility, payer, staffing, and risk controls are ready