Chronic Pain Management Clinic Startup Costs: $600K+ CAPEX

Key Takeaways
- Buildout CAPEX is $250,000, plus $15,000 monthly lease.
- Equipment and fixtures add $255,000 upfront.
- Technology setup totals $95,000 before subscriptions.
- Payroll, supplies, and marketing scale with revenue.
Estimate Startup Costs with Calculator
Startup CAPEX
Estimates capitalized startup assets for a chronic pain management clinic only.
Capex only This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, deposits, debt service, working capital, marketing, financing costs, and operating losses.
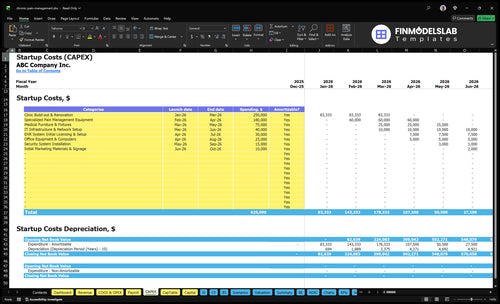
Does this screenshot show startup costs clearly?
Does this Chronic Pain Management Clinic Financial Model Template tab show startup CAPEX, expense categories, launch timing, costs, and depreciation or amortization? Review assumptions now.
Screenshot highlights
- CAPEX and buildout costs
- Launch timing and ramp
- Runway and staffing assumptions
What hidden costs do founders miss when starting a pain clinic?
The biggest hidden costs in a Chronic Pain Management Clinic are working capital, payer credentialing delays, malpractice and clinic insurance, compliance setup, billing setup, pre-opening payroll, training, supplies, and slow early collections; if you’re also sizing owner pay, see How Much Does The Owner Of Chronic Pain Management Clinic Typically Make Annually?. Working capital is not CAPEX, and Year 1 burn is heavy: $85,833/month payroll, $23,100/month fixed overhead, plus $1,800 EHR, $1,200 IT, $1,000 clinic insurance, and billing fees equal to 25% of Year 1 revenue.
Cash gaps to fund
- Working capital is a funding need.
- Credentialing delays slow payer cash.
- Early collections create cash gaps.
- Pre-opening payroll hits before revenue.
Run-rate costs
- $85,833/month Year 1 payroll.
- $23,100/month fixed overhead.
- $1,800 EHR, $1,200 IT.
- 25% of revenue goes to billing fees.
What financials do lenders need for funding a pain management clinic?
For a Chronic Pain Management Clinic, lenders want a clean funding pack that shows $600,000 in visible CAPEX, startup expenses, staffing, payer assumptions, reimbursement timing, revenue ramp, margins, break-even, and cash runway. The model should tie launch-period spend to buildout, equipment, EHR setup, and hiring, then show how $116,330 monthly Year 1 revenue can support $85,833 payroll, $23,100 fixed costs, and 145% revenue-linked costs without guessing at collection timing. With 51 million U.S. adults living with chronic pain, the lender case should prove demand and debt capacity, not hope.
Core lender package
- $600,000 CAPEX by launch period
- Startup expenses by month
- Staffing plan to opening day
- EHR setup and equipment timing
Repayment proof
- $116,330 Year 1 modeled monthly revenue
- $85,833 monthly payroll load
- $23,100 fixed costs each month
- Break-even and cash runway by payer mix
How much money do you need to open a pain management clinic?
You need more than $600,000 to open a Chronic Pain Management Clinic because visible CAPEX is only the starting point; cash must cover payroll and delays before reimbursements stabilize. For context, What Is The Key Indicator That Reflects The Success Of Chronic Pain Management Clinic? matters because over 51 million U.S. adults live with chronic pain, but demand does not remove working-capital risk.
Startup cash need
- Start above $600,000 visible CAPEX
- Size depends on clinic footprint
- Services drive equipment and staffing
- Payer mix drives cash timing
Year 1 pressure
- Revenue modeled at $116,330/month
- Wages plus overhead: $108,933/month
- Before 145% revenue-linked costs
- Team includes 6 clinical roles
Calculate Fuding Needs
Startup cost summary
This table summarizes startup asset costs plus the non-CAPEX cash reserve needed to open and survive the first operating months.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Clinic Build-out & Renovation | $250,000 | Tenant improvements and code-ready treatment space | Yes |
| Specialized Pain Management Equipment | $180,000 | Procedure and therapy equipment scope | Yes |
| Medical Furniture & Fixtures | $75,000 | Patient rooms, waiting area, and clinical fit-out | Yes |
| IT Infrastructure & Network Setup | $40,000 | Hardware, network, and clinic systems setup | Yes |
| EHR System Initial Licensing & Setup | $30,000 | Software license, setup, and onboarding | Yes |
| Working Capital Reserve | $338,000 | Month 12 cash trough from payroll and fixed overhead | No |
Chronic Pain Management Clinic Core Five Startup Costs
Facility And Clinical Buildout Startup Expense
Buildout Budget
$250,000 is set aside for clinic buildout and renovation from Month 1 through Month 3, while the facility lease runs at $15,000 per month starting in Month 1. Keep lease deposits and other pre-opening lease costs separate from capital spending (CAPEX) so your opening cash need is clear.
Space Scope
This budget covers exam rooms, treatment areas, procedure flow, waiting space, accessibility, plumbing, electrical, storage, and staff work areas. The estimate needs square footage, exam room count, and whether the clinic supports procedures or basic visits only.
- Count rooms before pricing
- Match layout to service mix
- Ask for local contractor quotes
Cost Control
Trim waste by sizing the build to the actual care model, not the wish list. A landlord allowance can offset tenant work, but only if it fits the lease terms. The big mistake is overbuilding for procedures you will not offer in year one.
- Price to current service scope
- Separate rent items from buildout
- Use standard finishes where possible
Sizing Inputs
Refine the estimate with square footage, procedure capability, landlord allowance, and local construction pricing. If the clinic adds image-guided procedures, plumbing, electrical load, and storage needs rise fast, so the floor plan should be locked before contractors start.
Medical Equipment And Procedure Asset Startup Expense
Furniture base
Your first split is furniture vs procedure gear. The supplied budget sets $75,000 for medical furniture and fixtures, which covers exam tables, chairs, desks, storage, and staff work areas. Size it from room count, square footage, and vendor quotes; a bigger footprint or more exam rooms pushes this line up fast.
Procedure gear
The $180,000 equipment budget is for specialized pain management assets: monitoring devices, treatment gear, procedure tools, and imaging-related items if you offer injections or image-guided care. Basic chronic pain visits need less than an interventional suite, so separate exam-room gear from procedure-room gear before pricing.
Buy in steps
The cleanest way to control this spend is to buy in phases. Start with the gear needed for your first services, then add imaging or procedure assets only when visit volume justifies them. The common mistake is overbuying for a future model that has not been staffed, credentialed, or booked yet.
Service mix drives CAPEX
A clinic built around counseling, nurse practitioner visits, and basic follow-up can stay lighter on assets than one offering injections or image-guided procedures. Physical therapy and acupuncture also change the equipment list, so map each service to its own room, tool, and quote before you lock the CAPEX plan.
Licensing, Compliance, Insurance, And Professional Setup Startup Expense
Compliance Setup
A chronic pain clinic needs entity formation, state clinic compliance, controlled-substance workflows, HIPAA policies, legal review, accounting setup, payer enrollment, malpractice coverage, and $1,000/month clinic insurance. State licensing and DEA needs vary by state and service mix, so budget from quotes, not guesses. Treat this as go-live infrastructure, not overhead you can defer.
Cost Drivers
Price this by state, service model, number of prescribers, and whether you handle controlled substances or procedures. Add months of malpractice and insurance coverage, payer enrollment work, and the time needed to build documentation standards. The biggest mistake is buying broad compliance support before the clinic scope is clear.
- Quote each state separately
- Map services before buying
- Enroll payers early
Keep It Tight
Trim cost by starting with the smallest service set you can document, bill, and supervise well. Use one clear workflow for prescribing, charting, and handoffs, then expand after payer files and audit checks are clean. Don’t cut HIPAA training, controlled-substance logs, or malpractice limits; that’s where pain clinics get expensive fast.
- Standardize templates first
- Delay scope creep
- Protect high-risk workflows
Risk Gate
For a clinic serving 51 million adults with chronic pain in the US, compliance protects both patients and collections. Tight documentation, clear prescribing rules, and clean payer files lower denial and audit risk, while weak controls can delay revenue and raise malpractice exposure. Build the process before the first patient, not after the first claim.
Clinical Technology And Revenue Cycle Startup Expense
Core tech spend
Clinical tech is a front-loaded cost: $30,000 for EHR licensing and setup, $40,000 for IT and network buildout, and $25,000 for computers and office gear. That’s $95,000 in CAPEX before opening. The stack should cover practice management, patient portal, scheduling, e-prescribing, PDMP checks, phones, and patient messaging.
What it covers
Estimate this from vendor quotes, user counts, device counts, and support months. The recurring layer is $1,800 per month for the EHR, $1,200 for IT support, plus billing fees at 25% of Year 1 revenue. Keep software subscriptions separate from hardware so the startup budget shows true cash needs.
- Count clinicians and front desk users.
- Quote setup, licenses, and support.
- Model fees as 0.25 × revenue.
Scope control
The main control is scope. Buy only the devices and modules needed for safe care, secure messaging, and clean claims work. The easy mistake is bundling every tool into EHR setup; that hides the real monthly burn of $3,000 before billing fees. Ask vendors to split implementation, subscription, and support on separate lines.
Monthly burn
Before any billing fee, recurring tech spend is $1,800 for EHR plus $1,200 for IT support, or $3,000 a month. Add billing system fees at 25% of Year 1 revenue, and revenue cycle discipline starts to matter as much as clinical volume and clean documentation.
Staffing, Supplies, And Launch Preparation Startup Expense
Payroll
Open with the full team costed at $1,030,000 in Year 1 payroll. That includes 1 interventional pain physician at $300,000, 2 physical therapists at $90,000 each, 1 psychologist counselor at $85,000, 1 nurse practitioner at $110,000, 1 acupuncturist at $70,000, 1 clinic manager at $95,000, 2 front desk staff at $45,000 each, and 2 medical assistants at $50,000 each. Start payroll before opening for recruiting, onboarding, and credentialing.
Supplies
Medical supplies run at 50% of revenue and pharmaceuticals at 30%, so cash need rises with volume, not headcount. Estimate stock as monthly treatments × unit cost, then add opening inventory for procedure kits, dressings, and office consumables. The marketing line is 40% of revenue, so launch spend can be heavy in Month 1.
Launch Prep
Launch prep is the work that makes day one usable: recruiting, onboarding, training, credentialing, front desk setup, and medical assistant workflow. Budget months, not days, because payer enrollment and clinical readiness can lag hiring. One clean rule: don’t open until rooms, phones, scheduling, and room-turn kits are ready.
Control
Cut cash burn by phasing hires and stocking only wha t the first procedure mix needs. The common mistake is buying full inventory before visit volume is proven. Better to stage payroll, confirm credentialing dates, and set reorder points from booked treatments so supplies and marketing stay tied to actual demand.
Compare 3 Startup Cost Scenarios
Scenario table
Startup cost rises with exam rooms, procedure gear, staffing, and cash runway. Lean, base, and full show the gap between consult-first, multidisciplinary, and interventional-heavy launches.
| Scenario | Lean LaunchConsult-first | Base LaunchMultidisciplinary | Full LaunchInterventional-heavy |
|---|---|---|---|
| Launch model | Start as a consult-first clinic with fewer rooms, lighter procedure use, and a shorter cash runway. | Launch with the Year 1 team and the model's visible CAPEX, then scale services as demand builds. | Build a larger interventional setup with more procedure capacity, more rooms, and a longer runway. |
| Typical setup | Few exam rooms, limited procedure gear, and lean support staffing. | Standard exam and treatment space, core procedure equipment, and the supplied Year 1 staffing mix. | More exam rooms, deeper procedure gear, expanded clinical space, and a larger support team. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | $450,000 - $750,000Lower cash need | $900,000 - $1,100,000Model baseline | $1,400,000 - $1,900,000Highest cash need |
| Best fit | Best for a consult-first operator testing demand before adding more procedures. | Best for a multidisciplinary clinic that wants the model's core service mix. | Best for an interventional-heavy group that wants more capacity from day one. |
Planning note: These ranges are researched planning assumptions from the model, not exact vendor quotes or live bids.
Related Products
- Chronic Pain Management Clinic Porter's Five Forces Analysis
- Chronic Pain Management Clinic BCG Matrix
- Chronic Pain Management Clinic Business Model Canvas
- 7 Financial and Operational KPIs for Chronic Pain Management Clinics
- Chronic Pain Management Clinic Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Chronic Pain Management Clinic Profit Margins
- How Much Does It Cost To Run A Chronic Pain Management Clinic Monthly?
- Chronic Pain Management Clinic Financial Model Template in Excel
- How Much Chronic Pain Management Clinic Owners Can Take Home: $351K–$651K
- How to Open a Chronic Pain Management Clinic in 4 to 9 Months
- How to Write a Chronic Pain Management Clinic Business Plan
- Chronic Pain Management Clinic Marketing Mix
- Chronic Pain Management Clinic Marketing Plan
- Chronic Pain Management Clinic Business Proposal
- Chronic Pain Management Clinic PESTEL Analysis
- Chronic Pain Management Clinic Pitch Deck Example Editable PPTX
- Chronic Pain Management Clinic Business SWOT Analysis
- Chronic Pain Management Clinic Value Proposition Canvas
Frequently Asked Questions
The supplied research shows at least $600,000 in visible CAPEX before working capital That includes $250,000 for buildout, $180,000 for specialized pain equipment, and $75,000 for medical furniture Total funding needed is higher because Year 1 payroll is about $85,833/month and fixed overhead is $23,100/month